Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Manual #1 FreeRange Poultry Farming (Table Egg and Inasal Meat Type Production)Dokument15 SeitenManual #1 FreeRange Poultry Farming (Table Egg and Inasal Meat Type Production)AndrewDonaire100% (1)
- Gemmotherapy For Everyone Extract PDFDokument26 SeitenGemmotherapy For Everyone Extract PDFHunor Ladó100% (1)
- ROUGHDokument19 SeitenROUGHSamadNoch keine Bewertungen
- Vitamins Report Usda 2015 PDFDokument35 SeitenVitamins Report Usda 2015 PDFsahtehesabmNoch keine Bewertungen
- PDHPE Core 2 Practice QuestionsDokument6 SeitenPDHPE Core 2 Practice Questionsdarcym2604Noch keine Bewertungen
- Cat Calm and Carry OnDokument4 SeitenCat Calm and Carry OnMaria PazNoch keine Bewertungen
- 5 Major Nutrition Program Groups (9.3.2019)Dokument5 Seiten5 Major Nutrition Program Groups (9.3.2019)André Battad FloresNoch keine Bewertungen
- Echocardiographic Phenotype of Canine Dilated Cardiomyopathy Differs Based On Diet TypeDokument9 SeitenEchocardiographic Phenotype of Canine Dilated Cardiomyopathy Differs Based On Diet TypeMiruna ChiriacNoch keine Bewertungen
- 28 Best Collagen Powder For Women Over 50 in 2023 Discover MagazineDokument1 Seite28 Best Collagen Powder For Women Over 50 in 2023 Discover MagazinevwddtsrfrzNoch keine Bewertungen
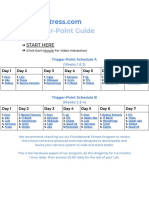
- 2.0 Trigger-Point Guide: Start HereDokument9 Seiten2.0 Trigger-Point Guide: Start HereBStrong Do No WrongNoch keine Bewertungen
- IronDokument27 SeitenIronAyman LatifNoch keine Bewertungen
- Vitamin and Mineral Supplementation During PregnanDokument4 SeitenVitamin and Mineral Supplementation During PregnanEvi RachmawatiNoch keine Bewertungen
- Enzymes & Probiotics Anticoccidials: CompositionDokument9 SeitenEnzymes & Probiotics Anticoccidials: CompositionKevin VoraNoch keine Bewertungen
- Drumstick Leaves Soup On Level of HaemoglobinDokument6 SeitenDrumstick Leaves Soup On Level of HaemoglobinAjay DNoch keine Bewertungen
- Procuct Brochure PDFDokument11 SeitenProcuct Brochure PDFspiritualbeing67% (3)
- Susan - Vitamin B12 Deficiency in EldersDokument15 SeitenSusan - Vitamin B12 Deficiency in Elderssoumya rahulNoch keine Bewertungen
- Hematological Indices of Pregnant Women Taking Iron - Folate Tablets PDFDokument42 SeitenHematological Indices of Pregnant Women Taking Iron - Folate Tablets PDFZeleke EndalewNoch keine Bewertungen
- 10-Ashique-2020-NaturalProductsBioprospecting-A Systemic Review On Topical MarketDokument21 Seiten10-Ashique-2020-NaturalProductsBioprospecting-A Systemic Review On Topical MarketGD & Hair ManagementNoch keine Bewertungen
- Week 11-2Dokument60 SeitenWeek 11-2Wong ChocolateNoch keine Bewertungen
- Thyroid Symptom Hacker - FINAL2Dokument18 SeitenThyroid Symptom Hacker - FINAL2Andreea IrinaNoch keine Bewertungen
- DaburDokument13 SeitenDaburSWETA GOGOI-DM 21DM205Noch keine Bewertungen
- Food and Nutrition: What Nourishes Our Children?Dokument9 SeitenFood and Nutrition: What Nourishes Our Children?Dorin FrunzaNoch keine Bewertungen
- Ujian Mid SemesterDokument6 SeitenUjian Mid SemesterTiffany PellengNoch keine Bewertungen
- Scitec Nutrition-Catalog 2011Dokument172 SeitenScitec Nutrition-Catalog 2011Relu VilcuNoch keine Bewertungen
- UC1 - Raise Organic ChickenDokument36 SeitenUC1 - Raise Organic ChickenButch DemayoNoch keine Bewertungen
- Nutritional Values in Shell and Flesh of The Giant Tiger Prawn Penaeus Monodon (Fabricius, 1798)Dokument4 SeitenNutritional Values in Shell and Flesh of The Giant Tiger Prawn Penaeus Monodon (Fabricius, 1798)International Journal of Current Innovations in Advanced ResearchNoch keine Bewertungen
- EctomorphDokument24 SeitenEctomorphbutt100% (7)
- Tridax Procumbens: A Prospective Bioactive Compound For Improving Men's Sexual HealthDokument2 SeitenTridax Procumbens: A Prospective Bioactive Compound For Improving Men's Sexual HealthmedtalksNoch keine Bewertungen
- Men Masculinity and Gendered AntiageingDokument20 SeitenMen Masculinity and Gendered AntiageingNesrin AydınNoch keine Bewertungen
- LWT Nutrition 2005Dokument22 SeitenLWT Nutrition 2005pawxblazerNoch keine Bewertungen