Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Gujral FCMDokument102 SeitenGujral FCMcandiddreamsNoch keine Bewertungen
- DM Infectious DiseasesDokument20 SeitenDM Infectious DiseasesVasishta NadellaNoch keine Bewertungen
- Maklumat Vaksinasi: Vaccination DetailsDokument2 SeitenMaklumat Vaksinasi: Vaccination Detailsbd sinarbarakahNoch keine Bewertungen
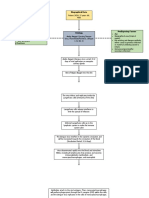
- Concept Map For DenvDokument4 SeitenConcept Map For Denvnikki sabs67% (3)
- Rinderpest (Cattle Plague) : Dr. Munguti E.M AHITI NdombaDokument14 SeitenRinderpest (Cattle Plague) : Dr. Munguti E.M AHITI NdombaFazalNoch keine Bewertungen
- Incubation Period: Jannah Marie A. Dimaporo - BIO030 (Section Uu)Dokument2 SeitenIncubation Period: Jannah Marie A. Dimaporo - BIO030 (Section Uu)Jannah Marie A. DimaporoNoch keine Bewertungen
- Ijmicro2020 6658445Dokument6 SeitenIjmicro2020 6658445Anika TahsinNoch keine Bewertungen
- Glenmark - Respicare: TEST PAPER - Microbiology, Disease, Organisms & AntibioticsDokument6 SeitenGlenmark - Respicare: TEST PAPER - Microbiology, Disease, Organisms & AntibioticskurutalaNoch keine Bewertungen
- Chapter 33: Atopic, Rheumatic, and Immunodeficiency Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokument8 SeitenChapter 33: Atopic, Rheumatic, and Immunodeficiency Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNoch keine Bewertungen
- Haemophilus and BordetellaDokument12 SeitenHaemophilus and BordetellaDaiki AomineNoch keine Bewertungen
- Agranulocytosis FinalDokument17 SeitenAgranulocytosis FinalsanthiyasandyNoch keine Bewertungen
- DS CD34 MicroBead Kit HDokument4 SeitenDS CD34 MicroBead Kit Hsankalpa3Noch keine Bewertungen
- Maape - Bacillary DysenteryDokument7 SeitenMaape - Bacillary Dysenterylorella_abejuelaNoch keine Bewertungen
- East-Mab IVD Products List20230608Dokument19 SeitenEast-Mab IVD Products List20230608ashutosh pandeyNoch keine Bewertungen
- Hepatitis B Profile InterpretationDokument43 SeitenHepatitis B Profile InterpretationSAMMYNoch keine Bewertungen
- Viral VaccinesDokument7 SeitenViral VaccinesMoon nieNoch keine Bewertungen
- Rheumatic Diseases Immunological Mechanisms and Prospects For New TherapiesDokument297 SeitenRheumatic Diseases Immunological Mechanisms and Prospects For New TherapiesАндрей ТихомировNoch keine Bewertungen
- Pneumonii Curs AMG 2018Dokument115 SeitenPneumonii Curs AMG 2018Ionut Horgot100% (2)
- Pathogenic Gram Positive BacteriaDokument34 SeitenPathogenic Gram Positive BacteriaFahimRazmandehNoch keine Bewertungen
- Bab 1Dokument1 SeiteBab 1sari murnaniNoch keine Bewertungen
- Agostino Bassi Elie Metchnikoff: Maestri-Coelia IshiwatariDokument1 SeiteAgostino Bassi Elie Metchnikoff: Maestri-Coelia IshiwatariSayantan ChoudhuryNoch keine Bewertungen
- Pajak PajakDokument13 SeitenPajak PajakrosyindahsariNoch keine Bewertungen
- IMMUNIZATION LecDokument77 SeitenIMMUNIZATION LecKavya ReddyNoch keine Bewertungen
- 4-Pathogenesis & Virulence LectureDokument25 Seiten4-Pathogenesis & Virulence Lecturetruch 2022Noch keine Bewertungen
- National Immunisation Program Schedule Queensland: February 2016Dokument2 SeitenNational Immunisation Program Schedule Queensland: February 2016Anonymous rLmr9GRM2Noch keine Bewertungen
- Module 2 PPDokument10 SeitenModule 2 PPAldous FajardoNoch keine Bewertungen
- Systemic Diseases Caused by Oral InfectionDokument12 SeitenSystemic Diseases Caused by Oral InfectionJing XueNoch keine Bewertungen
- Bns Accomplishment Report: Republic of The Philippines Province of Cavite Municipality of Amadeo Barangay PangilDokument2 SeitenBns Accomplishment Report: Republic of The Philippines Province of Cavite Municipality of Amadeo Barangay PangilelyssNoch keine Bewertungen
- Pathoma Notes CH 1-3Dokument11 SeitenPathoma Notes CH 1-3imdaking12392% (25)
- Scimagojr 2020Dokument2.453 SeitenScimagojr 2020heinz billNoch keine Bewertungen