Das könnte Ihnen auch gefallen
- Common Genetic Diseases-2548Dokument52 SeitenCommon Genetic Diseases-2548Veerapong VattanavanitNoch keine Bewertungen
- A Diagnostic Approach To Medias Tin UmDokument38 SeitenA Diagnostic Approach To Medias Tin UmVeerapong VattanavanitNoch keine Bewertungen
- ToxicologyDokument20 SeitenToxicologyVeerapong VattanavanitNoch keine Bewertungen
- Case Approach in HIV 29 Oct 2005Dokument222 SeitenCase Approach in HIV 29 Oct 2005Veerapong VattanavanitNoch keine Bewertungen
- TBDokument98 SeitenTBVeerapong VattanavanitNoch keine Bewertungen
- Diffuse Parenchymal Lung DiseaseDokument36 SeitenDiffuse Parenchymal Lung DiseaseVeerapong Vattanavanit100% (1)
- Ventilator Waveform AnalysisDokument96 SeitenVentilator Waveform AnalysisVeerapong Vattanavanit100% (11)
- VHDDokument69 SeitenVHDVeerapong VattanavanitNoch keine Bewertungen
- Interstitial Lung DiseasesDokument95 SeitenInterstitial Lung DiseasesVeerapong VattanavanitNoch keine Bewertungen
- SexDokument29 SeitenSexVeerapong VattanavanitNoch keine Bewertungen
- DMDokument30 SeitenDMVeerapong VattanavanitNoch keine Bewertungen
- Hematologic MalignancyDokument152 SeitenHematologic MalignancyVeerapong VattanavanitNoch keine Bewertungen
- SeizureDokument71 SeitenSeizureVeerapong Vattanavanit100% (1)
- AdrenalDokument27 SeitenAdrenalVeerapong VattanavanitNoch keine Bewertungen
- ElectrolyteDokument32 SeitenElectrolyteVeerapong VattanavanitNoch keine Bewertungen
- ParasiteDokument48 SeitenParasiteVeerapong Vattanavanit100% (1)
- HIV-Infected Patients Opportunistic Infections OverviewDokument53 SeitenHIV-Infected Patients Opportunistic Infections OverviewVeerapong VattanavanitNoch keine Bewertungen
- HIV-Infected Patients Opportunistic Infections OverviewDokument53 SeitenHIV-Infected Patients Opportunistic Infections OverviewVeerapong VattanavanitNoch keine Bewertungen
- 35ekg 1Dokument103 Seiten35ekg 1Veerapong Vattanavanit100% (2)
- Basic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalDokument79 SeitenBasic EKG 2: Dr. Wattana Wongtheptien M.D. Cardiologist Chiangrai Regional HospitalVeerapong Vattanavanit0% (1)
- HIV-Infected Patients Opportunistic Infections OverviewDokument53 SeitenHIV-Infected Patients Opportunistic Infections OverviewVeerapong VattanavanitNoch keine Bewertungen
- Review of Bacterial Infection SpecimenDokument45 SeitenReview of Bacterial Infection SpecimenVeerapong VattanavanitNoch keine Bewertungen
- HIV-Infected Patients Opportunistic Infections OverviewDokument53 SeitenHIV-Infected Patients Opportunistic Infections OverviewVeerapong VattanavanitNoch keine Bewertungen
- Urine Cast ดิวDokument40 SeitenUrine Cast ดิวVeerapong Vattanavanit100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
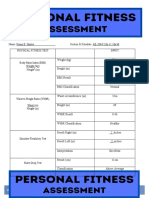
- Name: Kiano E. Santos Section & Schedule: AE-204/9:10a-11:10a M Physical Fitness Test InputDokument5 SeitenName: Kiano E. Santos Section & Schedule: AE-204/9:10a-11:10a M Physical Fitness Test InputKiano SantosNoch keine Bewertungen
- Food Junkies: Recovery From Food Addiction, 2nd Ed.: January 2019Dokument12 SeitenFood Junkies: Recovery From Food Addiction, 2nd Ed.: January 2019tecnologia- educativaNoch keine Bewertungen
- Nutrition Care ProcessDokument38 SeitenNutrition Care ProcessChristelle Kay AsisNoch keine Bewertungen
- CH 22 Chemical Coordination and IntegrationDokument4 SeitenCH 22 Chemical Coordination and IntegrationRohankanani007100% (1)
- 1st-Quarter - Exam-Physical Education and Health - Nature of Dance 12Dokument4 Seiten1st-Quarter - Exam-Physical Education and Health - Nature of Dance 12Erwin Louwee JoseNoch keine Bewertungen
- A Simplified Anabolic Burst Mass Gaining Program.Dokument8 SeitenA Simplified Anabolic Burst Mass Gaining Program.AliNoch keine Bewertungen
- The Science of Obesity Management: An Endocrine Society Scientific StatementDokument54 SeitenThe Science of Obesity Management: An Endocrine Society Scientific StatementLuminita HutanuNoch keine Bewertungen
- SL 5x5 Tracker LBDokument10 SeitenSL 5x5 Tracker LBBulgaricusNoch keine Bewertungen
- Self-Assess Health Fitness Status and DietDokument18 SeitenSelf-Assess Health Fitness Status and DietDonajei Rica100% (1)
- Animal Nutrition: For Campbell Biology, Ninth EditionDokument74 SeitenAnimal Nutrition: For Campbell Biology, Ninth EditionMahnoor AnjumNoch keine Bewertungen
- Why You'Re Not Losing Fat - 4 Hidden Mistakes You'Re Unknowingly MakingDokument14 SeitenWhy You'Re Not Losing Fat - 4 Hidden Mistakes You'Re Unknowingly Makingalejlcc100% (1)
- Activity LogDokument2 SeitenActivity LogMr Todd0% (1)
- Cardiorenal SyndromeDokument89 SeitenCardiorenal SyndromeGabriyah HamzahNoch keine Bewertungen
- What Is Physical FitnessDokument10 SeitenWhat Is Physical FitnessMaria Cassandra O. RamosNoch keine Bewertungen
- NutrastartDokument2 SeitenNutrastartapi-239680473Noch keine Bewertungen
- Q4Tday MAG2009 enDokument32 SeitenQ4Tday MAG2009 enJose ManuelNoch keine Bewertungen
- 1st Quarter Summative PE6 AssessmentDokument3 Seiten1st Quarter Summative PE6 AssessmentRonnie SumicadNoch keine Bewertungen
- Internacionalni Univerzitet Brčko Saobraćajni Fakultet Drumski SaobraćajDokument7 SeitenInternacionalni Univerzitet Brčko Saobraćajni Fakultet Drumski SaobraćajmevluwNoch keine Bewertungen
- Canada Board Mcqs Qualifing ExamDokument26 SeitenCanada Board Mcqs Qualifing Examdr47Noch keine Bewertungen
- LongevityDokument12 SeitenLongevitychai7750% (2)
- Mty1107 Sec9 Saquiton MF LipidsfornursingDokument8 SeitenMty1107 Sec9 Saquiton MF LipidsfornursingCes SaquitonNoch keine Bewertungen
- Body Mass Index (BMI) : What Does It Mean To Have A High BMI?Dokument2 SeitenBody Mass Index (BMI) : What Does It Mean To Have A High BMI?demmonNoch keine Bewertungen
- AI-powered Nutrition Analyzer For Fitness Enthusiasts - Problem StatementDokument2 SeitenAI-powered Nutrition Analyzer For Fitness Enthusiasts - Problem StatementGaneshkumarNoch keine Bewertungen
- Osteoporosis BrochureDokument2 SeitenOsteoporosis BrochurednllkzaNoch keine Bewertungen
- Thesis Final Na To (Maica)Dokument42 SeitenThesis Final Na To (Maica)John-Rey Prado100% (1)
- Algorithms For Data Science 1st Brian Steele (WWW - Ebook DL - Com)Dokument438 SeitenAlgorithms For Data Science 1st Brian Steele (WWW - Ebook DL - Com)Adj Gomez100% (8)
- Hypothyroid SymptomsDokument19 SeitenHypothyroid Symptomsfatima110100% (2)
- Australian Adult Pre Exercise Screening TextbookDokument58 SeitenAustralian Adult Pre Exercise Screening Textbookcarlos corteNoch keine Bewertungen
- Pendiq User Manual enDokument64 SeitenPendiq User Manual enMartin JoseNoch keine Bewertungen
- Pepsci RecallDokument3 SeitenPepsci RecallRumana AliNoch keine Bewertungen