Das könnte Ihnen auch gefallen
- Woolf: Inflation-Adjusted Spending Per Vermont PupilDokument1 SeiteWoolf: Inflation-Adjusted Spending Per Vermont PupilPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Family Characteristics by CountyDokument1 SeiteWoolf: Vermont Family Characteristics by CountyPhilip TortoraNoch keine Bewertungen
- Bernie Sanders Medical ReportDokument1 SeiteBernie Sanders Medical ReportPhilip TortoraNoch keine Bewertungen
- Woolf: Initial Claims For Unemployment InsuranceDokument1 SeiteWoolf: Initial Claims For Unemployment InsurancePhilip TortoraNoch keine Bewertungen
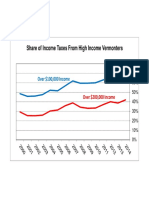
- Woolf: Share of Income Taxes From High Income VermontersDokument1 SeiteWoolf: Share of Income Taxes From High Income VermontersPhilip TortoraNoch keine Bewertungen
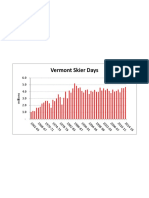
- Woolf: Vermont Skier DaysDokument1 SeiteWoolf: Vermont Skier DaysPhilip TortoraNoch keine Bewertungen
- Quinnipiac Presidential PollDokument9 SeitenQuinnipiac Presidential PollPhilip TortoraNoch keine Bewertungen
- Woolf: Number of Vermont Married CouplesDokument1 SeiteWoolf: Number of Vermont Married CouplesPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Earned Income Tax CreditDokument1 SeiteWoolf: Vermont Earned Income Tax CreditPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Labor Force and JobsDokument1 SeiteWoolf: Vermont Labor Force and JobsPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Gasoline and Fuel Oil PricesDokument1 SeiteWoolf: Vermont Gasoline and Fuel Oil PricesPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Median Family Income Jan 2016Dokument1 SeiteWoolf: Vermont Median Family Income Jan 2016Philip TortoraNoch keine Bewertungen
- Woolf: Vermont Labor Force & JobsDokument1 SeiteWoolf: Vermont Labor Force & JobsPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont PopulationDokument1 SeiteWoolf: Vermont PopulationPhilip TortoraNoch keine Bewertungen
- Affidavit: United States vs. Mark McLoudDokument9 SeitenAffidavit: United States vs. Mark McLoudPhilip TortoraNoch keine Bewertungen
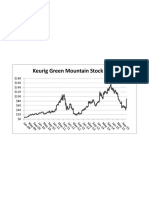
- Woolf: Keurig Green Mountain Stock PriceDokument1 SeiteWoolf: Keurig Green Mountain Stock PricePhilip TortoraNoch keine Bewertungen
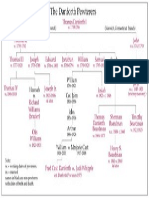
- The Danforth PewterersDokument1 SeiteThe Danforth PewterersPhilip TortoraNoch keine Bewertungen
- PDF: Northfield Fatal Fire Search Warrant ApplicationDokument10 SeitenPDF: Northfield Fatal Fire Search Warrant ApplicationPhilip TortoraNoch keine Bewertungen
- Woolf: Vermont Media Income by Household TypeDokument1 SeiteWoolf: Vermont Media Income by Household TypePhilip TortoraNoch keine Bewertungen
- Art Woolf: FY12 Vermont Government SpendingDokument1 SeiteArt Woolf: FY12 Vermont Government SpendingPhilip TortoraNoch keine Bewertungen
- Art Woolf: State and Local Taxes As A Share of Personal IncomeDokument1 SeiteArt Woolf: State and Local Taxes As A Share of Personal IncomePhilip TortoraNoch keine Bewertungen
- November 2012 Vaughan Real Estate Market UpdateDokument5 SeitenNovember 2012 Vaughan Real Estate Market Updateinfo7761Noch keine Bewertungen
- PDF: Court Papers Filed in Randy Quaid CaseDokument18 SeitenPDF: Court Papers Filed in Randy Quaid CasePhilip TortoraNoch keine Bewertungen
- Art Woolf: Percentage of Students Achieving A Score of Proficient or AdvancedDokument1 SeiteArt Woolf: Percentage of Students Achieving A Score of Proficient or AdvancedPhilip TortoraNoch keine Bewertungen
- Art Woolf: Vermont Payroll EmploymentDokument1 SeiteArt Woolf: Vermont Payroll EmploymentPhilip TortoraNoch keine Bewertungen
- Vermont State Police AMBER Alert ReviewDokument5 SeitenVermont State Police AMBER Alert ReviewPhilip TortoraNoch keine Bewertungen
- Art Woolf: Vermont Percent of Under 65 Population Without Health InsuranceDokument1 SeiteArt Woolf: Vermont Percent of Under 65 Population Without Health InsurancePhilip TortoraNoch keine Bewertungen
- Art Woolf: Vermont Construction EmploymentDokument1 SeiteArt Woolf: Vermont Construction EmploymentPhilip TortoraNoch keine Bewertungen
- PDF: Court Papers Filed in Evi Quaid CaseDokument23 SeitenPDF: Court Papers Filed in Evi Quaid CasePhilip TortoraNoch keine Bewertungen
- Art Woolf: Vermont Employment Change Since RecessionDokument1 SeiteArt Woolf: Vermont Employment Change Since RecessionPhilip TortoraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Data Sheet: High-Speed DiodesDokument7 SeitenData Sheet: High-Speed DiodesZoltán ÁgostonNoch keine Bewertungen
- PLTW: Digital Electronics Syllabus For Mrs. Yusufi: Unit 1: Fundamentals of Analog and DigitalDokument5 SeitenPLTW: Digital Electronics Syllabus For Mrs. Yusufi: Unit 1: Fundamentals of Analog and DigitalTriston DurbinNoch keine Bewertungen
- American With Disabilities Act AdaDokument16 SeitenAmerican With Disabilities Act Adaapi-376186426Noch keine Bewertungen
- Forensic Pharmacy: Dr. Zirwa AsimDokument35 SeitenForensic Pharmacy: Dr. Zirwa AsimZirwa AsimNoch keine Bewertungen
- CA 1 - Đề thi AV5 - CLC - Made - efDokument5 SeitenCA 1 - Đề thi AV5 - CLC - Made - efQuang NguyenNoch keine Bewertungen
- A Study To Assess The Effectiveness of PDokument9 SeitenA Study To Assess The Effectiveness of PKamal JindalNoch keine Bewertungen
- Explosive Ordnance DisposalDokument13 SeitenExplosive Ordnance DisposalZelwisNoch keine Bewertungen
- Physical Layer:: SwitchingDokument27 SeitenPhysical Layer:: SwitchingPKSachanNoch keine Bewertungen
- Advanced Blueprint 1Dokument3 SeitenAdvanced Blueprint 1api-728237431Noch keine Bewertungen
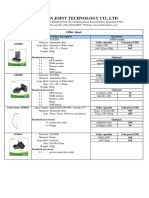
- Vehicle Tracker Offer SheetDokument1 SeiteVehicle Tracker Offer SheetBihun PandaNoch keine Bewertungen
- PC 5400 PC 5500Dokument53 SeitenPC 5400 PC 5500ArturHeiseNoch keine Bewertungen
- Katja Kruckeberg, Wolfgang Amann, Mike Green-Leadership and Personal Development - A Toolbox For The 21st Century Professional-Information Age Publishing (2011)Dokument383 SeitenKatja Kruckeberg, Wolfgang Amann, Mike Green-Leadership and Personal Development - A Toolbox For The 21st Century Professional-Information Age Publishing (2011)MariaIoanaTelecan100% (1)
- Creative WritingDokument2 SeitenCreative WritingSharmaine AsoyNoch keine Bewertungen
- 1 Clock Domain CrossingDokument35 Seiten1 Clock Domain CrossingRamakrishnaRao SoogooriNoch keine Bewertungen
- Veiga Et Al. 2015 - Composition, Structure and Floristic Diversity in Dense Rain Forest inDokument8 SeitenVeiga Et Al. 2015 - Composition, Structure and Floristic Diversity in Dense Rain Forest inYakov Mario QuinterosNoch keine Bewertungen
- The Advantages and Disadvantages If Block ChainDokument7 SeitenThe Advantages and Disadvantages If Block ChainKarthik ShettyNoch keine Bewertungen
- GbiDokument14 SeitenGbimaurice86Noch keine Bewertungen
- DUPLICATE BILL TITLEDokument8 SeitenDUPLICATE BILL TITLEMohammed AhmedNoch keine Bewertungen
- Test 420001 PDFDokument13 SeitenTest 420001 PDFmaria100% (1)
- List of Electronics Manufacturing Companies in Noida - ElectronicsmediaDokument2 SeitenList of Electronics Manufacturing Companies in Noida - ElectronicsmediaBlue Oceon50% (4)
- Lesson Plan 2 Sine Rule and Cosine RuleDokument8 SeitenLesson Plan 2 Sine Rule and Cosine Ruleapi-280114661Noch keine Bewertungen
- Physics Semiconductor Device MCQDokument3 SeitenPhysics Semiconductor Device MCQAsim Ali0% (1)
- 10 ExtSpringsDokument27 Seiten10 ExtSpringsresh27Noch keine Bewertungen
- Advances in X-Ray Analysis - Volume 33 - 1989Dokument685 SeitenAdvances in X-Ray Analysis - Volume 33 - 1989CVNoch keine Bewertungen
- Finimpianti Power EngDokument2 SeitenFinimpianti Power EngJosip GrlicaNoch keine Bewertungen
- Gmail LogoDokument12 SeitenGmail Logovinodram993480Noch keine Bewertungen
- IC-V80 V80E ManualDokument64 SeitenIC-V80 V80E Manualrzkyln100% (1)
- 102DNDokument2 Seiten102DNManuel ZavalaNoch keine Bewertungen
- Teodora Sarkizova: Certificate of AchievementDokument2 SeitenTeodora Sarkizova: Certificate of AchievementAbd El-RahmanNoch keine Bewertungen
- ME1001, ME1004, ME1005 - Basic Mech+Graphics+Workshop Pract.Dokument6 SeitenME1001, ME1004, ME1005 - Basic Mech+Graphics+Workshop Pract.Mayank AgarwalNoch keine Bewertungen