Das könnte Ihnen auch gefallen
- Acantholytic Solar Keratosis, M 67, Forehead PDFDokument6 SeitenAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous DiseaseDokument4 SeitenAcantholytic Bullous DiseaseDeba P SarmaNoch keine Bewertungen
- Accessory TragusDokument3 SeitenAccessory TragusDeba P SarmaNoch keine Bewertungen
- Pilar Cyst With CrystalsDokument2 SeitenPilar Cyst With CrystalsDeba P SarmaNoch keine Bewertungen
- Acantholytic Dermatosis With DyskeratosisDokument11 SeitenAcantholytic Dermatosis With DyskeratosisDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Dokument3 SeitenAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNoch keine Bewertungen
- Acantholytic Acanthoma. M 60, ScrotumDokument8 SeitenAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNoch keine Bewertungen
- Acantholytic Actinic KeratosisDokument4 SeitenAcantholytic Actinic KeratosisDeba P SarmaNoch keine Bewertungen
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Dokument6 SeitenBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNoch keine Bewertungen
- Results of Search in Google Scholar On 'Deba P Sarma'Dokument28 SeitenResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNoch keine Bewertungen
- Xanthogranuloma, M 30, Right ElbowDokument4 SeitenXanthogranuloma, M 30, Right ElbowDeba P SarmaNoch keine Bewertungen
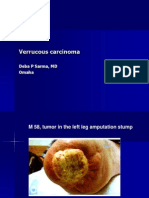
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDokument7 SeitenVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNoch keine Bewertungen
- Xanthogranuloma PPT DSDokument9 SeitenXanthogranuloma PPT DSDeba P SarmaNoch keine Bewertungen
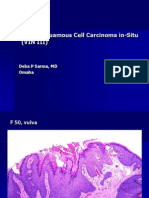
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDokument6 SeitenVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNoch keine Bewertungen
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDokument7 SeitenXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNoch keine Bewertungen
- Verrucous Epidermal Nevus. F 43, ScalpDokument4 SeitenVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNoch keine Bewertungen
- Verrucous Carcinoma of The Foot, M 63, Left FootDokument8 SeitenVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDokument2 SeitenVerruca Vulgaris., M 22.,PPTDeba P SarmaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Costeo Basado en ActividadesDokument11 SeitenCosteo Basado en Actividadesfrank richard lopez salinasNoch keine Bewertungen
- Pathology of Teeth and Supporting StructuresDokument45 SeitenPathology of Teeth and Supporting StructuresIsak ShatikaNoch keine Bewertungen
- Genital HerpesDokument2 SeitenGenital HerpesWisnu WardanaNoch keine Bewertungen
- COVID 19 Consent FormDokument2 SeitenCOVID 19 Consent FormfvdssfdNoch keine Bewertungen
- Merger Value CreationDokument11 SeitenMerger Value CreationAziz BouignaneNoch keine Bewertungen
- Pain and Pain Gate Control MechanismDokument17 SeitenPain and Pain Gate Control MechanismKapil LakhwaraNoch keine Bewertungen
- 3rd GenerationDokument3 Seiten3rd GenerationlorrainebarandonNoch keine Bewertungen
- EBOLADokument4 SeitenEBOLAwawa3385Noch keine Bewertungen
- Facilitator's Manual 2020 July 2020 FinalDokument176 SeitenFacilitator's Manual 2020 July 2020 Finalkaseera musaNoch keine Bewertungen
- Rhinitis Vasomotor Dek AmiDokument15 SeitenRhinitis Vasomotor Dek AmineviNoch keine Bewertungen
- Spectrum BrochureDokument16 SeitenSpectrum BrochuredimdamflyNoch keine Bewertungen
- Shamanism and Altered States of ConsciousnessDokument15 SeitenShamanism and Altered States of Consciousnessyodoid100% (2)
- Application of Pharmaceutical GelatinDokument4 SeitenApplication of Pharmaceutical GelatinShakrie AbdullahNoch keine Bewertungen
- OmronDokument19 SeitenOmrondekifps9893Noch keine Bewertungen
- GigaMune Rep-Seq Technical NoteDokument2 SeitenGigaMune Rep-Seq Technical NoteAndro HsuNoch keine Bewertungen
- Bihar Nursing HRH ReportDokument60 SeitenBihar Nursing HRH Reportachopra14Noch keine Bewertungen
- Concept Map Chap7 General Survey Vital SignsDokument1 SeiteConcept Map Chap7 General Survey Vital SignsEvelyn MoatsNoch keine Bewertungen
- Baumgaertner. The Value of The Tip-Apex Distance PDFDokument8 SeitenBaumgaertner. The Value of The Tip-Apex Distance PDFIcaruscignusNoch keine Bewertungen
- Pereneal CareDokument2 SeitenPereneal CareindumathiNoch keine Bewertungen
- Effectofcorestabilityexerciseonposturalstabilityinchildrenwith DownsyndromeDokument11 SeitenEffectofcorestabilityexerciseonposturalstabilityinchildrenwith Downsyndrome8 nocturnalNoch keine Bewertungen
- Pa2 and Pa3 2Dokument14 SeitenPa2 and Pa3 2Roger ViloNoch keine Bewertungen
- Anaesthesiology NAGY TESZTKÖNYVDokument1.064 SeitenAnaesthesiology NAGY TESZTKÖNYVoroszgabor100% (10)
- Common Pediatric Illnesses in The Er UrgentDokument46 SeitenCommon Pediatric Illnesses in The Er UrgentDr mohamedNoch keine Bewertungen
- New Eco Ink MsdsDokument7 SeitenNew Eco Ink MsdsankitleedsNoch keine Bewertungen
- Qi Presentation VapDokument19 SeitenQi Presentation Vapapi-383799988Noch keine Bewertungen
- Intensive Revision Course in Paediatrics (Poster)Dokument2 SeitenIntensive Revision Course in Paediatrics (Poster)Chris Jardine LiNoch keine Bewertungen
- Aluminum and Foam Sam Splint 2004+Dokument3 SeitenAluminum and Foam Sam Splint 2004+Ophelia PoppyNoch keine Bewertungen
- School of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareDokument13 SeitenSchool of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareSamjhana Neupane100% (1)
- Morphology of AcetabulumDokument14 SeitenMorphology of AcetabulumChee Wai HongNoch keine Bewertungen
- Guidelines For Good Clinical Practice in Clinical Trials (1998)Dokument49 SeitenGuidelines For Good Clinical Practice in Clinical Trials (1998)analyn123Noch keine Bewertungen