Das könnte Ihnen auch gefallen
- Mech1006 Materials & Mechanics: Metallography & Microstructure: Lab Session M, 2013, DR A WojcikDokument19 SeitenMech1006 Materials & Mechanics: Metallography & Microstructure: Lab Session M, 2013, DR A WojcikLoc Nguyen100% (1)
- Annual Performance Report 2012 (2019 2020)Dokument166 SeitenAnnual Performance Report 2012 (2019 2020)Abdilbasit Hamid75% (4)
- Olympus GF Type UCT180 User ManualDokument204 SeitenOlympus GF Type UCT180 User ManualJimena Lopez CardenasNoch keine Bewertungen
- Basic and Advanced Laboratory Techniques in Histopathology and CytologyDokument296 SeitenBasic and Advanced Laboratory Techniques in Histopathology and Cytologyjihann100% (2)
- NCRP Report 133 IndexDokument4 SeitenNCRP Report 133 IndexEng.AymanNoch keine Bewertungen
- Evaluation and Optimization of Laboratory Methods and Analytical ProceduresVon EverandEvaluation and Optimization of Laboratory Methods and Analytical ProceduresNoch keine Bewertungen
- Virtual Microscope by BIONETWORKDokument6 SeitenVirtual Microscope by BIONETWORKCrismar TakinanNoch keine Bewertungen
- Bionanotechnology - E. Papazoglou, A. Parthasarathy (2007) WWDokument148 SeitenBionanotechnology - E. Papazoglou, A. Parthasarathy (2007) WWbicarbonat100% (2)
- Treatment of Micropollutants in Water and WastewaterDokument11 SeitenTreatment of Micropollutants in Water and WastewateryenNoch keine Bewertungen
- Bio NanotechnologyDokument148 SeitenBio NanotechnologyDavid Lyons100% (1)
- Dispositivos de Diagnóstico in VitroDokument111 SeitenDispositivos de Diagnóstico in VitroKayo PaivaNoch keine Bewertungen
- Technical Guide: Sputum Examination For Tuberculosis by Direct Microscopy in Low Income CountriesDokument32 SeitenTechnical Guide: Sputum Examination For Tuberculosis by Direct Microscopy in Low Income CountriesMegan LewisNoch keine Bewertungen
- Lengkap PusingDokument52 SeitenLengkap PusingAyuNoch keine Bewertungen
- Odour Impacts Final-1Dokument145 SeitenOdour Impacts Final-1Absolute SteveNoch keine Bewertungen
- Review of Dioxins and Furan From Incineration CSRDokument216 SeitenReview of Dioxins and Furan From Incineration CSRJuliusNoch keine Bewertungen
- Non-Binding Guide To Good Practice For Implementing Directive 2006 25 ECDokument144 SeitenNon-Binding Guide To Good Practice For Implementing Directive 2006 25 ECmssmdocsNoch keine Bewertungen
- SpanacDokument127 SeitenSpanacTimothy BensonNoch keine Bewertungen
- PH Ysics: Manual For M.Sc. (P) Nuclear Physics LabDokument177 SeitenPH Ysics: Manual For M.Sc. (P) Nuclear Physics LabNishan RanabhatNoch keine Bewertungen
- The Intensive Care Unit MaualDokument356 SeitenThe Intensive Care Unit MaualMariefel Villanueva AlejagaNoch keine Bewertungen
- Smith Et Al 1996 Dose AssessmentDokument77 SeitenSmith Et Al 1996 Dose AssessmentReinel EchávezNoch keine Bewertungen
- Diss GarsuchDokument133 SeitenDiss GarsuchKhoa DuyNoch keine Bewertungen
- (Springer Protocols Handbooks) Mahin Basha - Analytical Techniques in Biochemistry-Springer US - Humana (2020)Dokument132 Seiten(Springer Protocols Handbooks) Mahin Basha - Analytical Techniques in Biochemistry-Springer US - Humana (2020)shuvvro dhaNoch keine Bewertungen
- Rezistenta Antimicrobiana in EuropaDokument208 SeitenRezistenta Antimicrobiana in EuropairiscelNoch keine Bewertungen
- ICRPDokument147 SeitenICRPGiovanni MateusNoch keine Bewertungen
- Mechanochemistry in Nanoscience and Minerals EngineeringDokument422 SeitenMechanochemistry in Nanoscience and Minerals EngineeringJazmin RuizNoch keine Bewertungen
- Handbook On Particle Separation Processes (2011) PDFDokument227 SeitenHandbook On Particle Separation Processes (2011) PDFmarmaduke32100% (1)
- Eng PDFDokument32 SeitenEng PDFMark Anthony MadridanoNoch keine Bewertungen
- ICU HandbookDokument146 SeitenICU HandbookBulent InanNoch keine Bewertungen
- Introduction To EDS AnalysisDokument53 SeitenIntroduction To EDS AnalysisDejan NaumovNoch keine Bewertungen
- Nano CrystalsDokument11 SeitenNano CrystalsTrần Lê Tuyết ChâuNoch keine Bewertungen
- Standards For Improving Quality of Maternaland Newborn Care in Health FacilitiesDokument84 SeitenStandards For Improving Quality of Maternaland Newborn Care in Health FacilitiesBettyUgazNoch keine Bewertungen
- The Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustDokument164 SeitenThe Intensive Care Unit at The Mid Yorkshire Hospitals NHS TrustRajiv Srinivasa71% (7)
- Protein Electrophoresis GEDokument82 SeitenProtein Electrophoresis GEIsa Ribeiro100% (1)
- Task Force ON Ritualistic Uses of MercuryDokument111 SeitenTask Force ON Ritualistic Uses of MercuryDr. John MichaelNoch keine Bewertungen
- Manual DVR BOLIDE MVR9008-3G UserDokument43 SeitenManual DVR BOLIDE MVR9008-3G UserJhonatan SepulvedaNoch keine Bewertungen
- CardiacDokument148 SeitenCardiacadel husseinNoch keine Bewertungen
- Chromatography of Mycotoxins: Techniques and ApplicationsVon EverandChromatography of Mycotoxins: Techniques and ApplicationsNoch keine Bewertungen
- Immunosensors For Detection of Pesticide ResiduesDokument11 SeitenImmunosensors For Detection of Pesticide Residuescatherine_henry-de-villeneuveNoch keine Bewertungen
- Guidance For Producing Safe Drinking-Water: ISBN 978 92 4 151277 0Dokument152 SeitenGuidance For Producing Safe Drinking-Water: ISBN 978 92 4 151277 0Grafi EinsteinNoch keine Bewertungen
- Corrosion Control in Drinking Water Distribution SystemsDokument65 SeitenCorrosion Control in Drinking Water Distribution SystemsSyavash EnshaNoch keine Bewertungen
- Guidelines For The Clinical Management of Severe Illness From Influenza Virus InfectionsDokument89 SeitenGuidelines For The Clinical Management of Severe Illness From Influenza Virus InfectionsNguyễn Thu TrangNoch keine Bewertungen
- Prescribing Recording and Reporting Brachytherapy For Cancer of 2013Dokument10 SeitenPrescribing Recording and Reporting Brachytherapy For Cancer of 2013sangeetha maniNoch keine Bewertungen
- IARC Monograph On EMF Radiation - No 102Dokument480 SeitenIARC Monograph On EMF Radiation - No 102mvannierNoch keine Bewertungen
- P Removal Design ManualDokument127 SeitenP Removal Design ManualKwang Je LeeNoch keine Bewertungen
- HandbookDokument143 SeitenHandbooksnakey666100% (2)
- National Pollutant Inventory Emission Estimation Technique Manual FORDokument78 SeitenNational Pollutant Inventory Emission Estimation Technique Manual FORGisselle VesgaNoch keine Bewertungen
- Optical Thin Films and Coatings 2E From Materials To Applications 2Nd Ed Edition Flory Download PDF ChapterDokument51 SeitenOptical Thin Films and Coatings 2E From Materials To Applications 2Nd Ed Edition Flory Download PDF Chaptermary.hanna173100% (5)
- Icrp 135Dokument144 SeitenIcrp 135Roshi_11Noch keine Bewertungen
- Paquet 2015Dokument188 SeitenPaquet 2015Nicholas AlmslawyNoch keine Bewertungen
- Radiotherapy: IPEM Grade A' Training PortfolioDokument9 SeitenRadiotherapy: IPEM Grade A' Training PortfoliorodricesarNoch keine Bewertungen
- Pollution Prevention: Methodology, Technologies and PracticesVon EverandPollution Prevention: Methodology, Technologies and PracticesNoch keine Bewertungen
- Immobilized pH Gradients: Theory and MethodologyVon EverandImmobilized pH Gradients: Theory and MethodologyNoch keine Bewertungen
- Uncertainty Analysis with High Dimensional Dependence ModellingVon EverandUncertainty Analysis with High Dimensional Dependence ModellingNoch keine Bewertungen
- Ophthalmic Viscoelastic Devices (OVD) in Ocular SurgeryVon EverandOphthalmic Viscoelastic Devices (OVD) in Ocular SurgeryNoch keine Bewertungen
- Platform Interference in Wireless Systems: Models, Measurement, and MitigationVon EverandPlatform Interference in Wireless Systems: Models, Measurement, and MitigationBewertung: 5 von 5 Sternen5/5 (1)
- CH 04 Lecture PresentationDokument55 SeitenCH 04 Lecture PresentationClayd Genesis CapadaNoch keine Bewertungen
- Lab 454 Practical 1Dokument18 SeitenLab 454 Practical 1Najihah OmarNoch keine Bewertungen
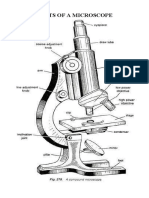
- Parts of A MicroscopeDokument5 SeitenParts of A MicroscopeShankey Faith BediaNoch keine Bewertungen
- Olympus Cx31Dokument23 SeitenOlympus Cx31Yudi FirmatiaNoch keine Bewertungen
- Risk Management and Laboratory SafetyDokument23 SeitenRisk Management and Laboratory SafetyChris Angelo De GuzmanNoch keine Bewertungen
- GENERALBIOLOGY1Q1MOD1Dokument12 SeitenGENERALBIOLOGY1Q1MOD1Shaira C. QuiselNoch keine Bewertungen
- Module 2 Elaborate Arial 12Dokument3 SeitenModule 2 Elaborate Arial 12eryan binsentNoch keine Bewertungen
- Microscopy: Course: MCB 103 Lab Section: 1 Name: Noor-E-Khadiza Shama ID: 1921168 Date: 28/01/20Dokument4 SeitenMicroscopy: Course: MCB 103 Lab Section: 1 Name: Noor-E-Khadiza Shama ID: 1921168 Date: 28/01/20ShamaNoch keine Bewertungen
- Labreport Exp2.1a2.2 g10Dokument9 SeitenLabreport Exp2.1a2.2 g10NUR NAJWA BINTI MOHD RAFIE MoeNoch keine Bewertungen
- Olympus CX31 Biological Microscope Manual PDFDokument24 SeitenOlympus CX31 Biological Microscope Manual PDFelnegro300Noch keine Bewertungen
- Prelab Activity MPLDokument5 SeitenPrelab Activity MPLAlthea Valenzuela100% (1)
- Leica DM-500 Microscope - User ManualDokument44 SeitenLeica DM-500 Microscope - User ManualluroguitaNoch keine Bewertungen
- LabManual 2012 PDFDokument346 SeitenLabManual 2012 PDFMaria PopNoch keine Bewertungen
- Thin Section MicrosDokument113 SeitenThin Section MicrosM Reza PahleviNoch keine Bewertungen
- Lecture-3 OMDokument61 SeitenLecture-3 OMarulmuruguNoch keine Bewertungen
- Biology Lab Manual MatriculationDokument104 SeitenBiology Lab Manual MatriculationNA MINoch keine Bewertungen
- Microscope Nikon OptiPhot ManualDokument32 SeitenMicroscope Nikon OptiPhot ManualstditamedNoch keine Bewertungen
- Chapter 3 Microsopy and Preparation of SpecimenDokument63 SeitenChapter 3 Microsopy and Preparation of SpecimenMARIAM AFIFAH NUBAHARINoch keine Bewertungen
- Microscopy-Principles and TypesDokument82 SeitenMicroscopy-Principles and TypesSELVI ANoch keine Bewertungen
- DB17-008 Various DiscontinuedDokument3 SeitenDB17-008 Various DiscontinuedMichael LopezNoch keine Bewertungen
- METU ENVE202 Laboratory ManualDokument47 SeitenMETU ENVE202 Laboratory ManualSarp ÇelebiNoch keine Bewertungen
- BIOL2103 Microbiology Manual (Updated Sept 2021)Dokument25 SeitenBIOL2103 Microbiology Manual (Updated Sept 2021)채연유Noch keine Bewertungen
- Practical Manual BIO 1141: University of Venda Department of Biological SciencesDokument42 SeitenPractical Manual BIO 1141: University of Venda Department of Biological SciencesBelfry MantshwaneNoch keine Bewertungen
- Cell Biology Practical 2 PDFDokument9 SeitenCell Biology Practical 2 PDFEswaran SingamNoch keine Bewertungen
- Exp 1 Bio Elab ManualDokument5 SeitenExp 1 Bio Elab ManualFATIN FARHANAH BINTI HALIDIN MoeNoch keine Bewertungen
- Veterinary Microbiology Laboratory Manua PDFDokument112 SeitenVeterinary Microbiology Laboratory Manua PDFrajkumar871992100% (1)
- Microscope ECLIPSE E200 InstructionsDokument62 SeitenMicroscope ECLIPSE E200 InstructionsIgnacio Candia Ramos0% (1)
- Histology Assignment 1Dokument3 SeitenHistology Assignment 1Kristine Pangahin100% (1)