Das könnte Ihnen auch gefallen
- Robbins Pathology Chapter 13 - White Blood CellsDokument7 SeitenRobbins Pathology Chapter 13 - White Blood Cellsscorpiosphinx7980% (5)
- 2009 Handbook of Nurse Anesthesia, John J. Nagelhout, Karen Plaus PDFDokument840 Seiten2009 Handbook of Nurse Anesthesia, John J. Nagelhout, Karen Plaus PDFNoval Zain100% (1)
- Clinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzDokument31 SeitenClinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzNoreenNoch keine Bewertungen
- Gross Anatomy Preliminary Exams SamplexDokument12 SeitenGross Anatomy Preliminary Exams SamplexCarlos NiñoNoch keine Bewertungen
- MBR Pathology Mock Exam 2021Dokument11 SeitenMBR Pathology Mock Exam 2021Shera Heart GoNoch keine Bewertungen
- Chapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFDokument12 SeitenChapter 8 Infectious Diseases Robbins and Cotran Pathologic Basis of Disease PDFRitz Celso100% (1)
- Robbin's SummariesDokument98 SeitenRobbin's SummariesnopedontsuemepleaseNoch keine Bewertungen
- Patho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Dokument12 SeitenPatho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Grant GarcesNoch keine Bewertungen
- Robbins Ch. 20 The Kidney Review QuestionsDokument10 SeitenRobbins Ch. 20 The Kidney Review QuestionsPA2014100% (4)
- PATHOLOGY Board Exam ANsWERSDokument22 SeitenPATHOLOGY Board Exam ANsWERSchristinejoan100% (1)
- CVS Essay QuestionsDokument3 SeitenCVS Essay QuestionsPeter AbikoyeNoch keine Bewertungen
- Ust Mock Boards 2017 - Anatomy-1Dokument10 SeitenUst Mock Boards 2017 - Anatomy-1Jason Mirasol100% (1)
- Pharmacology Trans 1Dokument4 SeitenPharmacology Trans 1GLOMARIE DE GUZMANNoch keine Bewertungen
- Chapter 11 Blood Vessels 8th Ed NotesDokument7 SeitenChapter 11 Blood Vessels 8th Ed NotesKyle Christopher SiaNoch keine Bewertungen
- 1.02 - Hemostasis, Surgical Bleeding and TransfusionsDokument11 Seiten1.02 - Hemostasis, Surgical Bleeding and TransfusionsPhilip Patrick LeeNoch keine Bewertungen
- PHYSIO Prelims SamplexDokument11 SeitenPHYSIO Prelims SamplexCarlos NiñoNoch keine Bewertungen
- (P) Ana - Uerm 2Dokument11 Seiten(P) Ana - Uerm 2Aj BrarNoch keine Bewertungen
- Physician's Licensure Exam. For Micro-ParaDokument4 SeitenPhysician's Licensure Exam. For Micro-ParaDonnaBells Hermo LabaniegoNoch keine Bewertungen
- MED1 Samplex Rationale 6 - Endocrine DisordersDokument6 SeitenMED1 Samplex Rationale 6 - Endocrine DisordersMartina GarciaNoch keine Bewertungen
- General PathologyDokument72 SeitenGeneral PathologyVishav JitNoch keine Bewertungen
- Pathology 1Dokument38 SeitenPathology 1ARNOLD BORROMEONoch keine Bewertungen
- Patho Supplement Handout For Sept 2018 UPDATED May 2018Dokument27 SeitenPatho Supplement Handout For Sept 2018 UPDATED May 2018emely p. tangoNoch keine Bewertungen
- Pathology Cell InjuryDokument57 SeitenPathology Cell InjuryMajd MustafaNoch keine Bewertungen
- Robbins - 12 The HeartDokument5 SeitenRobbins - 12 The HeartCM NajitoNoch keine Bewertungen
- General Pathology Bimonthly Exam Compilation Updated 2Dokument197 SeitenGeneral Pathology Bimonthly Exam Compilation Updated 2Cherry Rahima100% (1)
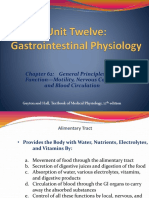
- Chapter 62: General Principles of GI Function-Motility, Nervous Control, and Blood CirculationDokument36 SeitenChapter 62: General Principles of GI Function-Motility, Nervous Control, and Blood Circulationjackie funtanillaNoch keine Bewertungen
- 14 Patho Head and Neck PathologyDokument10 Seiten14 Patho Head and Neck PathologyMartin TanNoch keine Bewertungen
- Biochemistry (1-20)Dokument30 SeitenBiochemistry (1-20)Stetho LoveNoch keine Bewertungen
- TOPNOTCH Parasitology-Supertable-by-Yns-Pereyra-Cocoy-Calderon-Troy-Soberano-UPDATED-NOVEMBER-2017Dokument25 SeitenTOPNOTCH Parasitology-Supertable-by-Yns-Pereyra-Cocoy-Calderon-Troy-Soberano-UPDATED-NOVEMBER-2017Waiwit KritayakiranaNoch keine Bewertungen
- Pathology Board QuestionsDokument86 SeitenPathology Board QuestionsJulius Matthew LuzanaNoch keine Bewertungen
- Liver - RobbinsDokument25 SeitenLiver - Robbinssarguss14100% (2)
- Tissue TableDokument4 SeitenTissue TableMarcie BooneNoch keine Bewertungen
- Neoplasia I - RecordingDokument6 SeitenNeoplasia I - RecordingIS99057Noch keine Bewertungen
- Pathology Ple SamplexDokument5 SeitenPathology Ple SamplexdawnparkNoch keine Bewertungen
- Parasite Trematodes PDFDokument2 SeitenParasite Trematodes PDFGougle MuteNoch keine Bewertungen
- Neuroanatomy SamplexDokument2 SeitenNeuroanatomy SamplexMineTagraNoch keine Bewertungen
- HEAD AND NECK 1.robbins & Cotran Pathologic Basis of Disease ReviewerDokument14 SeitenHEAD AND NECK 1.robbins & Cotran Pathologic Basis of Disease ReviewerSeff Causapin100% (1)
- Chapter 10 - Diseases of Infancy and ChildhoodDokument17 SeitenChapter 10 - Diseases of Infancy and ChildhoodAgnieszka WisniewskaNoch keine Bewertungen
- 1.embryology Q ADokument11 Seiten1.embryology Q ADr P N N ReddyNoch keine Bewertungen
- Helminth 5Dokument5 SeitenHelminth 5fiena92100% (2)
- 1 PATHO 2a - Inflammation - Dr. BailonDokument12 Seiten1 PATHO 2a - Inflammation - Dr. BailontonNoch keine Bewertungen
- (QUIZ) NEMATODES (2nd Year BS Medical Technology)Dokument2 Seiten(QUIZ) NEMATODES (2nd Year BS Medical Technology)avery aerNoch keine Bewertungen
- Final Coaching - Im 2022Dokument9 SeitenFinal Coaching - Im 2022Jhon PauloNoch keine Bewertungen
- 01 Physiology PLE 2019 Ratio1Dokument62 Seiten01 Physiology PLE 2019 Ratio1Patricia VillegasNoch keine Bewertungen
- Chapter 3 (Questions 2008-2009 Compiled)Dokument56 SeitenChapter 3 (Questions 2008-2009 Compiled)vetpathforumNoch keine Bewertungen
- Nematodes Quiz - MCQs With Answers - ProProfs QuizDokument1 SeiteNematodes Quiz - MCQs With Answers - ProProfs QuizHabtamu tamiruNoch keine Bewertungen
- AUB - Renal DiseasesDokument2 SeitenAUB - Renal DiseasesJeanne RodiñoNoch keine Bewertungen
- Divergent Differentiation, Creating So-Called Mixed Tumors: Seminoma Are Used For Malignant Neoplasms. TheseDokument6 SeitenDivergent Differentiation, Creating So-Called Mixed Tumors: Seminoma Are Used For Malignant Neoplasms. TheseSherwin Kenneth Madayag100% (1)
- Pedia MCUDokument65 SeitenPedia MCUfilchibuffNoch keine Bewertungen
- 08 Topnotch Surgery SuperExam - NOHIGHLIGHTSDokument94 Seiten08 Topnotch Surgery SuperExam - NOHIGHLIGHTSFrancine LucasNoch keine Bewertungen
- 03 Biochemistry PLE 2019 RatioDokument72 Seiten03 Biochemistry PLE 2019 RatioMae SimborioNoch keine Bewertungen
- Cellular ResponsesDokument19 SeitenCellular ResponsesFu Xiao ShanNoch keine Bewertungen
- Anatomy Compre Exams 2004 2005Dokument7 SeitenAnatomy Compre Exams 2004 2005GLeen Rose Onguda AguiLarNoch keine Bewertungen
- Patho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)Dokument13 SeitenPatho A 1. 3 Inflammation and Repair (Dy-Quiangco, 2015)kristineNoch keine Bewertungen
- Micro para Questions 2004 2005Dokument6 SeitenMicro para Questions 2004 2005DonnaBells Hermo LabaniegoNoch keine Bewertungen
- MBR 2019 - Radiology Handouts-Unlocked PDFDokument5 SeitenMBR 2019 - Radiology Handouts-Unlocked PDFCoy EnNoch keine Bewertungen
- Congestive Heart Failure, Cardiomyopathy and Myocarditis I. Congestive Heart FailureDokument23 SeitenCongestive Heart Failure, Cardiomyopathy and Myocarditis I. Congestive Heart Failurelovelyc95Noch keine Bewertungen
- Alterations in Cardiovascular FunctionsDokument191 SeitenAlterations in Cardiovascular FunctionsSheryll Joy Lopez CalayanNoch keine Bewertungen
- Cardio-Respiratory Conditions: by DR Priscus MushiDokument73 SeitenCardio-Respiratory Conditions: by DR Priscus MushiMusaNoch keine Bewertungen
- Acyanoticheartdiseases 180620040047 PDFDokument88 SeitenAcyanoticheartdiseases 180620040047 PDFElijahNoch keine Bewertungen
- Acyanoticheartdiseases 180620040047 PDFDokument88 SeitenAcyanoticheartdiseases 180620040047 PDFElijahNoch keine Bewertungen
- Medical Statistics Made Easy For The Medical PractDokument6 SeitenMedical Statistics Made Easy For The Medical PractLuming LiNoch keine Bewertungen
- World Happiness Report 2017Dokument188 SeitenWorld Happiness Report 2017Luming LiNoch keine Bewertungen
- Be It Enacted by The General Assembly of The State of ColoradoDokument15 SeitenBe It Enacted by The General Assembly of The State of ColoradoLuming LiNoch keine Bewertungen
- Checklist I: Graduates of New York State Registered or LCME/AOA-Accredited Programs (Domestic Graduates Not Using FCVS)Dokument3 SeitenChecklist I: Graduates of New York State Registered or LCME/AOA-Accredited Programs (Domestic Graduates Not Using FCVS)Luming LiNoch keine Bewertungen
- Bylaws of The Wayne State University Student Senate: MissionDokument22 SeitenBylaws of The Wayne State University Student Senate: MissionLuming LiNoch keine Bewertungen
- 2135Dokument321 Seiten2135Luming LiNoch keine Bewertungen
- McKinsey Roles For PhDsDokument2 SeitenMcKinsey Roles For PhDsLuming LiNoch keine Bewertungen
- End Arte Rec To MyDokument7 SeitenEnd Arte Rec To MyLuming LiNoch keine Bewertungen
- APD Recruiting TimelineDokument1 SeiteAPD Recruiting TimelineLuming LiNoch keine Bewertungen
- KKH Baby Bear Book 3rd EditionDokument672 SeitenKKH Baby Bear Book 3rd EditionJonathan TayNoch keine Bewertungen
- IVMS ICM-Heart MurmursDokument22 SeitenIVMS ICM-Heart MurmursMarc Imhotep Cray, M.D.Noch keine Bewertungen
- CardiomyopathyDokument1 SeiteCardiomyopathyTrisha VergaraNoch keine Bewertungen
- Peripartum Cardiomyopathy ReviewDokument14 SeitenPeripartum Cardiomyopathy ReviewWalter Saavedra Yarleque100% (1)
- Physical Examination FormDokument4 SeitenPhysical Examination FormDawit KumsaNoch keine Bewertungen
- MCPS Form For Annual Sports Physical Exam - (PPE) 2010 Edition Prepared by Am Academy of Ped, Am. Academy of Family Phys Et Al.Dokument5 SeitenMCPS Form For Annual Sports Physical Exam - (PPE) 2010 Edition Prepared by Am Academy of Ped, Am. Academy of Family Phys Et Al.Concussion_MCPS_MdNoch keine Bewertungen
- Cardiovascular Recommendation Tables PDFDokument38 SeitenCardiovascular Recommendation Tables PDFYesi Novia AmbaraniNoch keine Bewertungen
- Sudden Cardiac DeathDokument6 SeitenSudden Cardiac DeathdesindahNoch keine Bewertungen
- Pre-Participation Physical Evaluation Form (Ppe) : SignaturesDokument6 SeitenPre-Participation Physical Evaluation Form (Ppe) : Signatureskbarrier214Noch keine Bewertungen
- ICD 10 Penyakit KardiovaskularDokument20 SeitenICD 10 Penyakit KardiovaskularMaya ShofiaNoch keine Bewertungen
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDokument18 SeitenDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatePaloma GBNoch keine Bewertungen
- FacksheetDokument21 SeitenFacksheetFernandaNoch keine Bewertungen
- Evaluation MyocarditisDokument5 SeitenEvaluation MyocarditisRaidis PangilinanNoch keine Bewertungen
- CardiomyopathiesDokument48 SeitenCardiomyopathiesTanvir AhmedNoch keine Bewertungen
- Cardiology MnemonicsDokument18 SeitenCardiology MnemonicsAnnapurna Dangeti100% (1)
- Specified Illness Definitions GuideDokument46 SeitenSpecified Illness Definitions GuideRaja Nur Atiqah Hanim R Mohamad FaudziNoch keine Bewertungen
- UIL Safety TrainingDokument46 SeitenUIL Safety TrainingAnonymous iI88LtNoch keine Bewertungen
- Some PDFDokument55 SeitenSome PDFFred SmytheNoch keine Bewertungen
- Cardio My OpathiesDokument61 SeitenCardio My OpathiesIrina Cabac-PogoreviciNoch keine Bewertungen
- 6439-Article Text-59821-1-10-20231030Dokument12 Seiten6439-Article Text-59821-1-10-20231030Rakhmat RamadhaniNoch keine Bewertungen
- Evolving Indications For Permanent PacemakersDokument12 SeitenEvolving Indications For Permanent PacemakersJazmín Alejandra AGNoch keine Bewertungen
- Thesis Statement For Heart FailureDokument4 SeitenThesis Statement For Heart FailureWriteMyThesisPaperUK100% (1)
- Heart Failure: Definition and EpidemiologyDokument6 SeitenHeart Failure: Definition and EpidemiologyIshwarya SivakumarNoch keine Bewertungen
- 2019 Catheter Ablation of VA PDFDokument153 Seiten2019 Catheter Ablation of VA PDFyusupNoch keine Bewertungen
- Sas 13Dokument5 SeitenSas 13Sistine Rose LabajoNoch keine Bewertungen
- Introduction To Internal Medicine ........... 1:) 61) 62) 63 and Folate 63Dokument10 SeitenIntroduction To Internal Medicine ........... 1:) 61) 62) 63 and Folate 63sab kuch jano GNoch keine Bewertungen
- Polyclinic AllDokument92 SeitenPolyclinic AllFatima ShahNoch keine Bewertungen
- HEART FAILURE-WilliamDec (2005) PDFDokument602 SeitenHEART FAILURE-WilliamDec (2005) PDFChintya Fidelia MontangNoch keine Bewertungen
- Echo Heart FailureDokument82 SeitenEcho Heart FailureJing CruzNoch keine Bewertungen