Das könnte Ihnen auch gefallen
- Guidance IPE For NursingDokument57 SeitenGuidance IPE For NursingVitis Vini FeraNoch keine Bewertungen
- Brian Isetts, 2017, Integrating MTM Services Provided by Com PharmDokument12 SeitenBrian Isetts, 2017, Integrating MTM Services Provided by Com PharmVitis Vini FeraNoch keine Bewertungen
- WHO HRH HPN 10.3 EngDokument64 SeitenWHO HRH HPN 10.3 EngArif Eko YuniawanNoch keine Bewertungen
- The Attitudes of Medical Nursing and Pharmacy S 2011 Procedia Social andDokument7 SeitenThe Attitudes of Medical Nursing and Pharmacy S 2011 Procedia Social andVitis Vini FeraNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Top Chemists in Matunga East, MumbaiDokument6 SeitenTop Chemists in Matunga East, MumbaiSubhrajeet TalukdarNoch keine Bewertungen
- Lab 9 RespitatoryDokument3 SeitenLab 9 RespitatoryanaNoch keine Bewertungen
- Past Exam PaperDokument5 SeitenPast Exam PaperDavid Le50% (2)
- BDS 2nd Year DM NotesDokument34 SeitenBDS 2nd Year DM NotesPUBG VS FREE FIRENoch keine Bewertungen
- Contoh Tabel Stock OpnameDokument6 SeitenContoh Tabel Stock Opnamenadya hermawanNoch keine Bewertungen
- Drug interactions with diazepam reviewDokument7 SeitenDrug interactions with diazepam reviewAnonymous JvptVyNsNoch keine Bewertungen
- MHT Cet Bpharmacy Cap Round 1 All India Cutoff 2022Dokument16 SeitenMHT Cet Bpharmacy Cap Round 1 All India Cutoff 2022Aniket AgvaneNoch keine Bewertungen
- Price List AllDokument9 SeitenPrice List Alliimsaim saimNoch keine Bewertungen
- Patient Understanding of Dispensed Drugs at TBGH 2022 Final ResearchDokument60 SeitenPatient Understanding of Dispensed Drugs at TBGH 2022 Final ResearchIbrahimNoch keine Bewertungen
- BIOCONDokument11 SeitenBIOCONAravind SairamNoch keine Bewertungen
- Orphan DrugsDokument14 SeitenOrphan DrugsLeah BralowNoch keine Bewertungen
- ASHP Guidelines For Selecting PharmaceuticalDokument2 SeitenASHP Guidelines For Selecting PharmaceuticalKita RadisaNoch keine Bewertungen
- Danny's ResumeDokument2 SeitenDanny's ResumeDanny McLainNoch keine Bewertungen
- UCM285145 Responding To Unsolicited Requests For Off-Label Information About Prescription Drugs and Medical DevicesDokument15 SeitenUCM285145 Responding To Unsolicited Requests For Off-Label Information About Prescription Drugs and Medical DevicesJames LindonNoch keine Bewertungen
- Regulations of Pharmacovigilance in AzerbaijanDokument19 SeitenRegulations of Pharmacovigilance in AzerbaijanFaisal Mohammed Shamim KhanNoch keine Bewertungen
- Pakistan Pharmaceutical Industry Challenges & Future ProspectsDokument30 SeitenPakistan Pharmaceutical Industry Challenges & Future ProspectsarifmukhtarNoch keine Bewertungen
- Biowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidDokument15 SeitenBiowaiver Monograph For Immediate-Release Solid Oral Dosage Forms: Acetylsalicylic AcidPasinduAlwisNoch keine Bewertungen
- Refresher Course For Registered PharmacistDokument1 SeiteRefresher Course For Registered PharmacistThe Unknown 97Noch keine Bewertungen
- Oktober 2021Dokument150 SeitenOktober 2021farmasi rspcNoch keine Bewertungen
- Types of Drug Utilization StudiesDokument14 SeitenTypes of Drug Utilization StudiesFyrrNoch keine Bewertungen
- Avelino Activity3bDokument3 SeitenAvelino Activity3bDebbie S. AvelinoNoch keine Bewertungen
- 08.07.2021. Shift III - Depo ICUDokument126 Seiten08.07.2021. Shift III - Depo ICUAri SaputraNoch keine Bewertungen
- 54 Tables of Anti Infecti 2015 Mandell Douglas and Bennett S PrinciplesDokument78 Seiten54 Tables of Anti Infecti 2015 Mandell Douglas and Bennett S PrinciplesHelen DyNoch keine Bewertungen
- Nama Obat/Barang Satuan No. ID Jenis Barang Keluar Jan 2022 Keluar Jan 2023Dokument27 SeitenNama Obat/Barang Satuan No. ID Jenis Barang Keluar Jan 2022 Keluar Jan 2023CitrahsnNoch keine Bewertungen
- 16.MDR-XDR TBDokument18 Seiten16.MDR-XDR TBLinna SriwaningsiNoch keine Bewertungen
- Tablets LfyDokument1 SeiteTablets Lfyadrian perezNoch keine Bewertungen
- RF FVDB-05 Application For Veterinary Drug and Product Registration (CPR)Dokument5 SeitenRF FVDB-05 Application For Veterinary Drug and Product Registration (CPR)jeffrey ignacioNoch keine Bewertungen
- Price List NovemberDokument280 SeitenPrice List NovemberEvans SobbaNoch keine Bewertungen
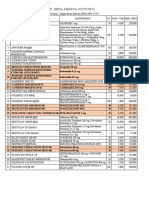
- PT.RIAU ANDALAN FARMA inventory reportDokument25 SeitenPT.RIAU ANDALAN FARMA inventory reportVannyNoch keine Bewertungen
- Pharma Handouts Rev 3Dokument34 SeitenPharma Handouts Rev 3Aphrill Pearl PacisNoch keine Bewertungen