Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Alinker R-Volution Walking BicycleDokument30 SeitenThe Alinker R-Volution Walking Bicyclerhend5Noch keine Bewertungen
- Mamdani Fuzzy Inference System Application Setting For Traffic LightsDokument7 SeitenMamdani Fuzzy Inference System Application Setting For Traffic LightsInternational Journal of Application or Innovation in Engineering & ManagementNoch keine Bewertungen
- Chaguetmi-Derradji2020 Article AssessmentOfTheEnvironmentalQuDokument26 SeitenChaguetmi-Derradji2020 Article AssessmentOfTheEnvironmentalQuMeriem MerioumaNoch keine Bewertungen
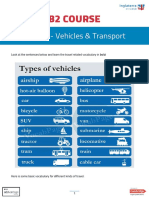
- B2 Course: Unit 48 - Vehicles & TransportDokument6 SeitenB2 Course: Unit 48 - Vehicles & TransportEugeniaNoch keine Bewertungen
- A History of PedestrianDokument8 SeitenA History of PedestrianHuswantoro AnggitNoch keine Bewertungen
- Argumentative EssayDokument6 SeitenArgumentative EssayAmber NicosiaNoch keine Bewertungen
- Road Safety Audit ManualDokument32 SeitenRoad Safety Audit ManualAbdullah Abdel-MaksoudNoch keine Bewertungen
- CH 5 Hill RoadDokument42 SeitenCH 5 Hill RoadSujan Singh100% (3)
- Design and Construction of Joints For Concrete Streets: Jointing ConsiderationsDokument12 SeitenDesign and Construction of Joints For Concrete Streets: Jointing ConsiderationsluftwachNoch keine Bewertungen
- PrEN 12271 - Surface DressingDokument54 SeitenPrEN 12271 - Surface DressingPedjaNoch keine Bewertungen
- Traffic ManagementDokument66 SeitenTraffic ManagementZubaida KilinaNoch keine Bewertungen
- LTODokument6 SeitenLTOKeeben Letrero BadoyNoch keine Bewertungen
- Traffic Modelling GuidelinesDokument585 SeitenTraffic Modelling Guidelinesebinsams007Noch keine Bewertungen
- Traffic Signs in The PhilippinesDokument39 SeitenTraffic Signs in The PhilippinesRamil BillonesNoch keine Bewertungen
- Initial Environmental Examination (Iee) Checklist: 1. General InformationDokument15 SeitenInitial Environmental Examination (Iee) Checklist: 1. General InformationavieNoch keine Bewertungen
- Qatar Traffic AwarnessDokument9 SeitenQatar Traffic AwarnesshardavNoch keine Bewertungen
- Murum To Akkalkot - Main Report - Volume I of XIDokument241 SeitenMurum To Akkalkot - Main Report - Volume I of XIHemendra JasaparaNoch keine Bewertungen
- Otmp Mainscript 05072004Dokument19 SeitenOtmp Mainscript 05072004bhaskarNoch keine Bewertungen
- How To Give Directions in English Instructions Exa Classroom Posters Conversation Topics Dialogs Fun - 120678Dokument5 SeitenHow To Give Directions in English Instructions Exa Classroom Posters Conversation Topics Dialogs Fun - 120678Maria joseNoch keine Bewertungen
- 02 Fundamentals of Junction DesignDokument84 Seiten02 Fundamentals of Junction DesignBrian PaulNoch keine Bewertungen
- Zenia F Saraswati - TransportationDokument14 SeitenZenia F Saraswati - TransportationM ADNAN ZNoch keine Bewertungen
- Risk Assessment For Installation of Sanitary WaresDokument14 SeitenRisk Assessment For Installation of Sanitary WaresAnandu Ashokan67% (6)
- Preparation: (H) Ead - Literature SuppositoryDokument237 SeitenPreparation: (H) Ead - Literature SuppositoryIllegal Pad Publishing100% (2)
- Actual Semi Truck Complaint SampleDokument10 SeitenActual Semi Truck Complaint SampleShirley WeissNoch keine Bewertungen
- 9 Basic Competency Driving NC IIDokument57 Seiten9 Basic Competency Driving NC IIrecquelle danoNoch keine Bewertungen
- TDC-15-S-06 Driver's Duties and ResponsibilitiesDokument43 SeitenTDC-15-S-06 Driver's Duties and ResponsibilitiesJerry Cane60% (5)
- Volume I Cts For mmr-0909Dokument569 SeitenVolume I Cts For mmr-0909api-270998557100% (1)
- Automatic Raising BollardsDokument26 SeitenAutomatic Raising BollardsK SubramaniNoch keine Bewertungen
- NCHRP RPT 492 PDFDokument77 SeitenNCHRP RPT 492 PDFScott FergusonNoch keine Bewertungen
- Traffic Light Control System Design Using Omron PLC With Ladder Diagram MethodDokument7 SeitenTraffic Light Control System Design Using Omron PLC With Ladder Diagram MethodUgh AhhNoch keine Bewertungen