Das könnte Ihnen auch gefallen
- Academy For Five Element Acupuncture Catalog 2013Dokument72 SeitenAcademy For Five Element Acupuncture Catalog 2013Shari Blake40% (5)
- The Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2Dokument288 SeitenThe Cervical & Thoracic Spine - Mechanical Diagnosis & Therapy - Vol 2booksbearreading100% (6)
- Airway Management - AdultDokument13 SeitenAirway Management - AdultD M Shawkot HossainNoch keine Bewertungen
- Encephalitis Case StudyDokument83 SeitenEncephalitis Case Studymonica50% (4)
- Asthma Nursing Care Plans - LippincottDokument45 SeitenAsthma Nursing Care Plans - LippincottDyllanoNoch keine Bewertungen
- Lyme DiseaseDokument133 SeitenLyme Diseaseernestval100% (3)
- '05 Sullivan A.Dokument48 Seiten'05 Sullivan A.Geo NavarroNoch keine Bewertungen
- DR Lim Meng Lang Manual TemplateDokument25 SeitenDR Lim Meng Lang Manual TemplatedrtshNoch keine Bewertungen
- DR Lim Meng Lang Manual TemplateDokument25 SeitenDR Lim Meng Lang Manual TemplatedrtshNoch keine Bewertungen
- Chronic Kidney DiseaseDokument12 SeitenChronic Kidney DiseaseRoseben SomidoNoch keine Bewertungen
- Cardiac Biomarkers: Muhammad Shoaib Ph.D. ScholarDokument53 SeitenCardiac Biomarkers: Muhammad Shoaib Ph.D. ScholarMuhammad ShoaibNoch keine Bewertungen
- NICU Protocol 100Dokument76 SeitenNICU Protocol 100Catherine Lee100% (1)
- Aidet FinalDokument11 SeitenAidet Finalapi-273608948100% (1)
- Patient Satisfaction SurveyDokument3 SeitenPatient Satisfaction SurveyGlady Jane TevesNoch keine Bewertungen
- Present-Tratamentul in DislipidemieDokument52 SeitenPresent-Tratamentul in DislipidemieAdina BrahaNoch keine Bewertungen
- Elderly Skin CareDokument46 SeitenElderly Skin CareRobbyNoch keine Bewertungen
- New Developments in The Management of Dyslipidemia: Widjanarko. W MDDokument62 SeitenNew Developments in The Management of Dyslipidemia: Widjanarko. W MDyulanda fitrianaNoch keine Bewertungen
- Statins in CVD Management: Is Just Lipid Lowering Enough?Dokument37 SeitenStatins in CVD Management: Is Just Lipid Lowering Enough?SriNoch keine Bewertungen
- Atorvastatin Statin in CVD ManagementDokument37 SeitenAtorvastatin Statin in CVD ManagementSriNoch keine Bewertungen
- 1 s2.0 S0735109722064920 MainDokument2 Seiten1 s2.0 S0735109722064920 MainRapee JarungsirawatNoch keine Bewertungen
- Acute Myocard Ial Infarction in Young AdultDokument57 SeitenAcute Myocard Ial Infarction in Young Adultshafiyah82Noch keine Bewertungen
- New Developments in The Management of DyslipidemiaDokument63 SeitenNew Developments in The Management of DyslipidemiaM Azmi HNoch keine Bewertungen
- CvotDokument29 SeitenCvotakash kondapalliNoch keine Bewertungen
- HHS Public AccessDokument15 SeitenHHS Public AccessThành Nguyễn VănNoch keine Bewertungen
- RosuvastatinDokument62 SeitenRosuvastatinEileen del RosarioNoch keine Bewertungen
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDokument18 SeitenGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiNoch keine Bewertungen
- 0900 0920 Antiplatelet and Anticoaulation Therapy Aleti FINALDokument31 Seiten0900 0920 Antiplatelet and Anticoaulation Therapy Aleti FINALMarcelliaNoch keine Bewertungen
- Cardiac PanelDokument6 SeitenCardiac Panellinjinxian444Noch keine Bewertungen
- Lecture 25 - Plasma Ins 3 - 2006Dokument31 SeitenLecture 25 - Plasma Ins 3 - 2006api-3703352Noch keine Bewertungen
- Cardiovascular Disease and Dyslipidemia: Beyond LDLDokument10 SeitenCardiovascular Disease and Dyslipidemia: Beyond LDLGuillen CelisNoch keine Bewertungen
- Newer Biomarkers of ACSDokument89 SeitenNewer Biomarkers of ACSHafeesh FazuluNoch keine Bewertungen
- Millllllaaa 123Dokument11 SeitenMillllllaaa 123200742 Elya AmaliaNoch keine Bewertungen
- 2019 Dyslipidemia Guideline EscDokument30 Seiten2019 Dyslipidemia Guideline EscBubu ToNoch keine Bewertungen
- Cardiac Function Test 2018Dokument35 SeitenCardiac Function Test 2018Chandana Padma Priya JuturNoch keine Bewertungen
- The Grey Zone: What To Do For The "Intermediate Risk" Patient?Dokument96 SeitenThe Grey Zone: What To Do For The "Intermediate Risk" Patient?Shweta GajreNoch keine Bewertungen
- Jurnal Kardio 2Dokument6 SeitenJurnal Kardio 2Gaby YosephineNoch keine Bewertungen
- BOWO - The Impact of New Medications Guideline To The Diabetes Guideline EditDokument31 SeitenBOWO - The Impact of New Medications Guideline To The Diabetes Guideline EditReynalth SinagaNoch keine Bewertungen
- Wos Care LipidDokument55 SeitenWos Care LipidJuliana FeronNoch keine Bewertungen
- Management of Blood Cholesterol 2019Dokument2 SeitenManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNoch keine Bewertungen
- CRP PPT RealDokument16 SeitenCRP PPT RealShuaibu bukhariNoch keine Bewertungen
- Guidelines On The Use of Biochemical Cardiac Markers and Risk FactorsDokument39 SeitenGuidelines On The Use of Biochemical Cardiac Markers and Risk FactorsAbdalla ShaboNoch keine Bewertungen
- " Hypercholesterolemia: Pathophysiology and Therapeutics" "Hypercholesterolemia: Pathophysiology and Therapeutics"Dokument7 Seiten" Hypercholesterolemia: Pathophysiology and Therapeutics" "Hypercholesterolemia: Pathophysiology and Therapeutics"kookiescreamNoch keine Bewertungen
- Cardiac BiomarkersDokument32 SeitenCardiac BiomarkersMaham RehmanNoch keine Bewertungen
- Pathfast BrochureDokument6 SeitenPathfast BrochureJacky Junaedi100% (1)
- Association Between Baseline LDL-C Level and TotalDokument14 SeitenAssociation Between Baseline LDL-C Level and TotalMr. LNoch keine Bewertungen
- Mller Bardorff2000Dokument9 SeitenMller Bardorff2000Daniel ChaNoch keine Bewertungen
- Jurnal 2Dokument5 SeitenJurnal 2Nova SipahutarNoch keine Bewertungen
- 3 - Statin Primary Secondary MelaDokument57 Seiten3 - Statin Primary Secondary MelaKurniadin YayanNoch keine Bewertungen
- 1 s2.0 S0735109716366992 mmc1Dokument10 Seiten1 s2.0 S0735109716366992 mmc1Pangala NitaNoch keine Bewertungen
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDokument13 SeitenEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNoch keine Bewertungen
- Comparative Effects of LO-mg Versus 80-Mg Atorvastatin On High-Sensitivity C-Reactive ProteinDokument16 SeitenComparative Effects of LO-mg Versus 80-Mg Atorvastatin On High-Sensitivity C-Reactive ProteinferdianriskaNoch keine Bewertungen
- Tapan Debnath, Sankar Roy, Biswajit Majumdar, Avik Chakraborty, Partha Sarathi Pal and Mohan Chandra MondalDokument5 SeitenTapan Debnath, Sankar Roy, Biswajit Majumdar, Avik Chakraborty, Partha Sarathi Pal and Mohan Chandra MondalVia RahmahNoch keine Bewertungen
- Stroke Topic DiscussionDokument19 SeitenStroke Topic Discussionapi-648714317Noch keine Bewertungen
- Cardiac BiomarDokument34 SeitenCardiac BiomarVaibhav KaroliyaNoch keine Bewertungen
- Methods For Measuremnent of LDL CholesterolDokument19 SeitenMethods For Measuremnent of LDL Cholesterolmaheren tubeNoch keine Bewertungen
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDokument65 SeitenLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranNoch keine Bewertungen
- Narsum 1 Tatalaksana DislipidemiaDokument32 SeitenNarsum 1 Tatalaksana DislipidemiabimaNoch keine Bewertungen
- Treatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlideDokument31 SeitenTreatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlidejoshuaNoch keine Bewertungen
- Ann Soehee - Tctap2021 - SPCDokument43 SeitenAnn Soehee - Tctap2021 - SPCSaad KhanNoch keine Bewertungen
- Jurnal 4 WordDokument20 SeitenJurnal 4 WordSri MaryatiNoch keine Bewertungen
- Cardiac Troponin: Prof. Adi Koesoema AmanDokument58 SeitenCardiac Troponin: Prof. Adi Koesoema Amanbudi darmantaNoch keine Bewertungen
- Raza2004 PDFDokument12 SeitenRaza2004 PDFIvana RuseskaNoch keine Bewertungen
- 2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolDokument113 Seiten2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolIris GzlzNoch keine Bewertungen
- Reference Values Lab Tests Cardiac Profile Tests 3 PgsDokument3 SeitenReference Values Lab Tests Cardiac Profile Tests 3 PgsJim Varghese100% (1)
- C Reaktive ProteinDokument4 SeitenC Reaktive Proteinsinggih2008Noch keine Bewertungen
- Cardiac Biomarkers: When To Test? - Physician Perspective: Review ArticleDokument5 SeitenCardiac Biomarkers: When To Test? - Physician Perspective: Review ArticleShaoran AuliaNoch keine Bewertungen
- Jurnal MaglitinideDokument7 SeitenJurnal MaglitinideWanda Novia P SNoch keine Bewertungen
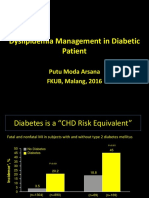
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Dokument31 SeitenDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaNoch keine Bewertungen
- The 2013 ACC/AHA Cholesterol Guidelines: What Do They Mean and How Should They Affect Practice?Dokument48 SeitenThe 2013 ACC/AHA Cholesterol Guidelines: What Do They Mean and How Should They Affect Practice?RovanNoch keine Bewertungen
- Accepted Manuscript: 10.1016/j.jacl.2017.02.017Dokument34 SeitenAccepted Manuscript: 10.1016/j.jacl.2017.02.017ochaNoch keine Bewertungen
- Shish Ehb or 703Dokument7 SeitenShish Ehb or 703Fadel Rajab NugrahaNoch keine Bewertungen
- TX LipidosDokument14 SeitenTX Lipidosxander trujilloNoch keine Bewertungen
- 2009 KK Talk JupiterDokument30 Seiten2009 KK Talk JupiterdrtshNoch keine Bewertungen
- Festival of LightsDokument413 SeitenFestival of LightsdrtshNoch keine Bewertungen
- SPMPS QuotationsDokument11 SeitenSPMPS Quotationsdrtsh100% (1)
- DR Lim Meng Lang Manual Template UpdatedDokument26 SeitenDR Lim Meng Lang Manual Template Updateddrtsh100% (4)
- DR John Chew (SPMPS President) PresentationDokument50 SeitenDR John Chew (SPMPS President) PresentationdrtshNoch keine Bewertungen
- Dr. S R Manalan's PresentationDokument58 SeitenDr. S R Manalan's Presentationdrtsh100% (1)
- Ms Chai's Presentation "Checklist On Self-Inspection of Private Clinics"Dokument33 SeitenMs Chai's Presentation "Checklist On Self-Inspection of Private Clinics"drtshNoch keine Bewertungen
- Right & Responsibility of Private Medical PractitionerDokument21 SeitenRight & Responsibility of Private Medical PractitionerdrtshNoch keine Bewertungen
- DR Lim Meng LangDokument49 SeitenDR Lim Meng LangdrtshNoch keine Bewertungen
- June IssueDokument8 SeitenJune IssuedrtshNoch keine Bewertungen
- The Basal Ganglia and Movement Disorders 2015 RevisedDokument19 SeitenThe Basal Ganglia and Movement Disorders 2015 RevisedJoan ChoiNoch keine Bewertungen
- Investigation and Treatment of Surgical JaundiceDokument38 SeitenInvestigation and Treatment of Surgical JaundiceUjas PatelNoch keine Bewertungen
- Flick ResumeDokument6 SeitenFlick ResumekellieNoch keine Bewertungen
- Electro ArticlesDokument21 SeitenElectro ArticlesZeaan SainNoch keine Bewertungen
- Tumori Tesuturi MoiDokument123 SeitenTumori Tesuturi MoiOana BarbuNoch keine Bewertungen
- Group MediclaimDokument21 SeitenGroup MediclaimAishwarya Deepak ChintalapatiNoch keine Bewertungen
- Normal GFR in ChildDokument8 SeitenNormal GFR in ChildbobbypambudimdNoch keine Bewertungen
- 2 CP Bekam Angin Tahap 3Dokument8 Seiten2 CP Bekam Angin Tahap 3Norhissam MustafaNoch keine Bewertungen
- Bisecting and Parelling TechniqueDokument32 SeitenBisecting and Parelling TechniqueArka Saha100% (1)
- Cochlear KansoDokument64 SeitenCochlear KansoSoumya RampalNoch keine Bewertungen
- PMDT Referrals - Ver 2Dokument15 SeitenPMDT Referrals - Ver 2Mark Johnuel DuavisNoch keine Bewertungen
- Texas Has The Highest Maternal Mortality Rate in The Developed WorldDokument5 SeitenTexas Has The Highest Maternal Mortality Rate in The Developed WorldDixanetNoch keine Bewertungen
- Complications of Peptic Ulcer Disease: Surgical ManagementDokument57 SeitenComplications of Peptic Ulcer Disease: Surgical ManagementJoan LuisNoch keine Bewertungen
- KSRR 24 201Dokument7 SeitenKSRR 24 201Jesiree DizonNoch keine Bewertungen
- Alternativas A TotalesDokument12 SeitenAlternativas A TotalesJuan Jose Stuven RodriguezNoch keine Bewertungen
- Kuliah 8. Anestesi - Syok Dan Tata LaksananyaDokument63 SeitenKuliah 8. Anestesi - Syok Dan Tata LaksananyaDesi Suryani DewiNoch keine Bewertungen
- Clinical Instrumentation, MLT 2760, BCC, Assessment Test 2Dokument9 SeitenClinical Instrumentation, MLT 2760, BCC, Assessment Test 2alphacetaNoch keine Bewertungen