Das könnte Ihnen auch gefallen
- Sample Competency Assessment ToolDokument10 SeitenSample Competency Assessment ToolHengkyNoch keine Bewertungen
- Scripps Hospital Patient Visitor Policy PDFDokument2 SeitenScripps Hospital Patient Visitor Policy PDFcode4saleNoch keine Bewertungen
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsVon EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNoch keine Bewertungen
- Infection Prevention and Control Assessment Tool For Outpatient SettingsDokument22 SeitenInfection Prevention and Control Assessment Tool For Outpatient SettingsVera IndrawatiNoch keine Bewertungen
- Ways To Improve The Health SystemDokument18 SeitenWays To Improve The Health SystemB I N SNoch keine Bewertungen
- Hospital Infection Control: Cecilia S. Montalban, MD, MSCCTMDokument51 SeitenHospital Infection Control: Cecilia S. Montalban, MD, MSCCTMDelantar Percivic100% (1)
- Self Assessment ToolkitDokument54 SeitenSelf Assessment ToolkitshekarNoch keine Bewertungen
- Out Patient DepartmentDokument5 SeitenOut Patient DepartmentShikhaNoch keine Bewertungen
- Handout Core CompetenciesDokument4 SeitenHandout Core CompetenciesAi CaNoch keine Bewertungen
- Incident Policy - Mercy Hospital NZDokument16 SeitenIncident Policy - Mercy Hospital NZoptical420Noch keine Bewertungen
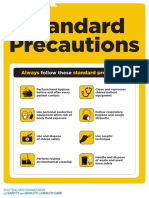
- Approach 4 Standard Precautions Icon PDF 672KBDokument1 SeiteApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaNoch keine Bewertungen
- 2018 JCI Sentinel - Event - Policy1 PDFDokument5 Seiten2018 JCI Sentinel - Event - Policy1 PDFAhmedNoch keine Bewertungen
- Hospital Safety PromotionDokument46 SeitenHospital Safety PromotionRhodora BenipayoNoch keine Bewertungen
- Policies On Continue Interval To Act An Orders For TreatmentDokument197 SeitenPolicies On Continue Interval To Act An Orders For TreatmentMk Salamat Remoquillo100% (1)
- Out Patient CareDokument20 SeitenOut Patient CarePan SoapNoch keine Bewertungen
- Who Patient SafetyDokument14 SeitenWho Patient SafetyJuwita Valen RamadhanniaNoch keine Bewertungen
- Disaster Management PlanDokument14 SeitenDisaster Management PlanpriyaNoch keine Bewertungen
- Vital Signs and Early Warning ScoresDokument47 SeitenVital Signs and Early Warning Scoresdr_nadheem100% (1)
- JCI Accreditation Presentation 4Dokument53 SeitenJCI Accreditation Presentation 4Osama MarzoukNoch keine Bewertungen
- Perspectives of Nursing Theory - An Overview: L. Anand Lecturer, College of Nursing, Neigrihms, ShillongDokument22 SeitenPerspectives of Nursing Theory - An Overview: L. Anand Lecturer, College of Nursing, Neigrihms, ShillongVũ Nguyễn Quỳnh TrangNoch keine Bewertungen
- Health Care and The Market Class NotesDokument16 SeitenHealth Care and The Market Class NotessmartisaacNoch keine Bewertungen
- No Such Thing As Ethical Organ MarketDokument3 SeitenNo Such Thing As Ethical Organ MarketRandae WuffyoteNoch keine Bewertungen
- NHI4UHC Day 4 Session 7 Partnering For Health Insurance: The Abu Dhabi ExperienceDokument12 SeitenNHI4UHC Day 4 Session 7 Partnering For Health Insurance: The Abu Dhabi ExperienceADB Health Sector Group100% (1)
- CHA Hospital Activation of The Emergency Operations Plan ChecklistDokument5 SeitenCHA Hospital Activation of The Emergency Operations Plan Checklistraysub159Noch keine Bewertungen
- Surgical Site Marking PolicyDokument11 SeitenSurgical Site Marking PolicymiraNoch keine Bewertungen
- M.B.A Hospital ManagementDokument42 SeitenM.B.A Hospital ManagementArun MuruganNoch keine Bewertungen
- Topic 5 (Chumaira Anindayudina)Dokument8 SeitenTopic 5 (Chumaira Anindayudina)Nndaydna100% (1)
- Strategies To Improve Handoff CommunicationDokument2 SeitenStrategies To Improve Handoff CommunicationJames SimmonsNoch keine Bewertungen
- Disaster ManagementDokument5 SeitenDisaster ManagementVedita ShelarNoch keine Bewertungen
- 2007 International Patient Safety GoalsDokument1 Seite2007 International Patient Safety GoalsElias Baraket FreijyNoch keine Bewertungen
- Define Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalDokument15 SeitenDefine Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalAbdul RahamanNoch keine Bewertungen
- Emergency DepartmentDokument25 SeitenEmergency DepartmentphanikrNoch keine Bewertungen
- Quality AssuranceDokument43 SeitenQuality Assurancekanika100% (1)
- Revised Guidelines For Air Conditioning in Operation TheatresDokument6 SeitenRevised Guidelines For Air Conditioning in Operation TheatresSaba RahmanNoch keine Bewertungen
- Continuing Education CalendarDokument76 SeitenContinuing Education CalendarBNoch keine Bewertungen
- Patient Support AreasDokument22 SeitenPatient Support AreasVivienne Rozenn LaytoNoch keine Bewertungen
- Brenda Creaney PresentationDokument21 SeitenBrenda Creaney Presentationmonir61Noch keine Bewertungen
- Civil Hospital Karachi Emergency PlanDokument25 SeitenCivil Hospital Karachi Emergency Plandr_bhuttoNoch keine Bewertungen
- Central Triage ProtocolDokument1 SeiteCentral Triage Protocolgechworkneh38Noch keine Bewertungen
- Clinical LeadershipDokument16 SeitenClinical LeadershipShiller MaroufzadehNoch keine Bewertungen
- Emergency Departement in Aiyiyah Mother and Child HospitalDokument3 SeitenEmergency Departement in Aiyiyah Mother and Child HospitalHida Tri NurrochmahNoch keine Bewertungen
- 2.1. Organising For SafetyDokument29 Seiten2.1. Organising For SafetyPERATCHI SELVANNoch keine Bewertungen
- IC 13 Guidelines On Standards For High Dependency UnitsDokument4 SeitenIC 13 Guidelines On Standards For High Dependency UnitsAnonymous 0WHX7nNoch keine Bewertungen
- VCT ManualDokument70 SeitenVCT ManualNay Lin HtikeNoch keine Bewertungen
- JD Ward Clerk Job DescriptionDokument2 SeitenJD Ward Clerk Job DescriptionMD Luthfy LubisNoch keine Bewertungen
- Central Sterile Supply Department: Mallikarjuna MHADokument25 SeitenCentral Sterile Supply Department: Mallikarjuna MHAsandhyakrishnanNoch keine Bewertungen
- Flow Chart For Adult Cardio-Pulmonary Resuscitation (Adult CPR)Dokument1 SeiteFlow Chart For Adult Cardio-Pulmonary Resuscitation (Adult CPR)Lia IshakNoch keine Bewertungen
- Clarification On Fire SafetyDokument1 SeiteClarification On Fire SafetyNaviin KrishnanNoch keine Bewertungen
- British Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyDokument6 SeitenBritish Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyPriscilla CarmiolNoch keine Bewertungen
- Administration of Hospital Admissions and Discharges PolicyDokument4 SeitenAdministration of Hospital Admissions and Discharges PolicyGillan TeravosaNoch keine Bewertungen
- Missing Patients ProcedureDokument16 SeitenMissing Patients ProcedureAgnieszka WaligóraNoch keine Bewertungen
- Quality Records: Neptune OrthopaedicsDokument1 SeiteQuality Records: Neptune Orthopaedicsdhir.ankurNoch keine Bewertungen
- Disaster MGMTDokument72 SeitenDisaster MGMTVarinder PalNoch keine Bewertungen
- Executive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentDokument5 SeitenExecutive Summary On Bio-Medical Waste Management: Quantitative Techniques and Research Methods in Management AssignmentMayuri VarkeyNoch keine Bewertungen
- Monograph of Qi ProjectDokument29 SeitenMonograph of Qi ProjectmerahiNoch keine Bewertungen
- Clinical Practice in AmbulanceDokument4 SeitenClinical Practice in Ambulancengurah_wardanaNoch keine Bewertungen
- Fiscal PlanningDokument22 SeitenFiscal PlanningRadha Sri100% (2)
- Data CollectionDokument30 SeitenData CollectionHarihara PuthiranNoch keine Bewertungen
- Patient Safety Organization A Complete Guide - 2020 EditionVon EverandPatient Safety Organization A Complete Guide - 2020 EditionNoch keine Bewertungen