Das könnte Ihnen auch gefallen
- Hallandale, FL33009 Tel: 954-457-8898 Fax: 954-457-8809Dokument4 SeitenHallandale, FL33009 Tel: 954-457-8898 Fax: 954-457-8809Katherine AcevedoNoch keine Bewertungen
- Cases MSDokument16 SeitenCases MSTessa GibsonNoch keine Bewertungen
- Fascial Distortion Model - Vol.4Dokument76 SeitenFascial Distortion Model - Vol.4Magno FilhoNoch keine Bewertungen
- Assignment McqsDokument13 SeitenAssignment Mcqsfaria ashrafNoch keine Bewertungen
- Neuromuscular Disorders: Peripheral Nervous System/ Myelopathy Case SessionDokument3 SeitenNeuromuscular Disorders: Peripheral Nervous System/ Myelopathy Case Sessionamitm2012Noch keine Bewertungen
- Chronic Psoas Syndrome Caused by The Inappropriate Use of A Heel Lift PDFDokument4 SeitenChronic Psoas Syndrome Caused by The Inappropriate Use of A Heel Lift PDFTito AlhoNoch keine Bewertungen
- 1Dokument1 Seite1shemeshjNoch keine Bewertungen
- UzemaDokument7 SeitenUzemaShawn DavisNoch keine Bewertungen
- Case PresentationDokument19 SeitenCase PresentationIbad Ur RehmanNoch keine Bewertungen
- Cervical Radiculopathy With Neurological DeficitDokument5 SeitenCervical Radiculopathy With Neurological DeficitHager salaNoch keine Bewertungen
- SCS Chapter02Dokument25 SeitenSCS Chapter02dawnNoch keine Bewertungen
- Lower Limb Anatomy PBLDokument3 SeitenLower Limb Anatomy PBLFrancesca vitaleNoch keine Bewertungen
- Ankle PainnDokument4 SeitenAnkle PainngoodlucksonkiloNoch keine Bewertungen
- Osteosarcoma CaseDokument2 SeitenOsteosarcoma CaseMarizz SamoyNoch keine Bewertungen
- A Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- A Case Study of Cauda Equina SyndromeDokument5 SeitenA Case Study of Cauda Equina SyndromeProfessor Stephen D. Waner100% (5)
- Individual Work 15Dokument5 SeitenIndividual Work 15Nur Fatima SanaaniNoch keine Bewertungen
- Health and Homeostasis 1 Assessment Task 1: Clinical Case Scenario AnalysisDokument4 SeitenHealth and Homeostasis 1 Assessment Task 1: Clinical Case Scenario AnalysismaureenNoch keine Bewertungen
- An Unusual Cause of Knee Pain Discovered at A Nurse Practitioner ClinicDokument5 SeitenAn Unusual Cause of Knee Pain Discovered at A Nurse Practitioner ClinicFajar MuhammadNoch keine Bewertungen
- Sample Documents For Medical ScribeDokument3 SeitenSample Documents For Medical ScribeMeghal SivanNoch keine Bewertungen
- Scolioza CongenitalaDokument20 SeitenScolioza CongenitalaIulia Dulgheru100% (1)
- 2002 5 206 209 PDFDokument4 Seiten2002 5 206 209 PDFlapogunevasNoch keine Bewertungen
- Sciatica and The Sacroiliac JointDokument4 SeitenSciatica and The Sacroiliac JointfilipecorsairNoch keine Bewertungen
- Clinical Cases NeurologyDokument200 SeitenClinical Cases Neurologysimi y100% (1)
- 3 s2.0 B9780443067167000074 MainDokument3 Seiten3 s2.0 B9780443067167000074 MainKarthik BhashyamNoch keine Bewertungen
- Manual Therapy: Rebecca Nelson, Toby HallDokument5 SeitenManual Therapy: Rebecca Nelson, Toby HallDiego SubiabreNoch keine Bewertungen
- Clinical Decision Making To Determine Need For Medical ReferralDokument12 SeitenClinical Decision Making To Determine Need For Medical ReferralaroobaNoch keine Bewertungen
- Neurologist MyChart - Visit Summary 2Dokument5 SeitenNeurologist MyChart - Visit Summary 2Iffat khanNoch keine Bewertungen
- Pamj 41 17Dokument10 SeitenPamj 41 17Sakib AhammadNoch keine Bewertungen
- CRS OsteomielitisDokument65 SeitenCRS OsteomielitisckaterineNoch keine Bewertungen
- PTH 725 - Multiple-Sclerosis-Case StudyDokument19 SeitenPTH 725 - Multiple-Sclerosis-Case StudyEnrique Guillen InfanteNoch keine Bewertungen
- Artigo - JoelhoDokument4 SeitenArtigo - JoelhoizabellegoesNoch keine Bewertungen
- 9th Week Orthopedic Disorders Case ScenarioDokument1 Seite9th Week Orthopedic Disorders Case ScenarioManarNoch keine Bewertungen
- NMS CasesDokument7 SeitenNMS CasesIgn_SkyfangNoch keine Bewertungen
- Case Study On Lower Cross Syndrome.Dokument2 SeitenCase Study On Lower Cross Syndrome.MRITUNJAY KUMAR SHARMANoch keine Bewertungen
- September1988CSBeazell PDFDokument2 SeitenSeptember1988CSBeazell PDFkotzaNoch keine Bewertungen
- Pid OrthoDokument9 SeitenPid OrthosapphireNoch keine Bewertungen
- TetrapareseDokument38 SeitenTetraparesemariamunsriNoch keine Bewertungen
- Osteophyte at The Sacroiliac JointDokument4 SeitenOsteophyte at The Sacroiliac JointHayyu F RachmadhanNoch keine Bewertungen
- FMcase 10Dokument14 SeitenFMcase 10Ryan TownsendNoch keine Bewertungen
- A Rare Case of Illiopsoas Weakness in A Woman After Delevery-The Effect of PhysiotherapyDokument4 SeitenA Rare Case of Illiopsoas Weakness in A Woman After Delevery-The Effect of PhysiotherapyayadandiaNoch keine Bewertungen
- S: Chief Complaint: "My Left Shoulder Hurts." Health History: Patient Denies Any History of Neurological DisordersDokument2 SeitenS: Chief Complaint: "My Left Shoulder Hurts." Health History: Patient Denies Any History of Neurological DisordersBlake RennerNoch keine Bewertungen
- CWU AttirahDokument13 SeitenCWU AttirahMuhammad HaziqNoch keine Bewertungen
- Villalon GRCaudaEquina2PRDokument12 SeitenVillalon GRCaudaEquina2PRpaul villalonNoch keine Bewertungen
- Cwu Ortho TraumaDokument9 SeitenCwu Ortho TraumaMia MusNoch keine Bewertungen
- DystrophyDokument3 SeitenDystrophyzbhabhaNoch keine Bewertungen
- Report of CaseDokument3 SeitenReport of CasefransAPNoch keine Bewertungen
- Physical Examination: Orthopedics: Clinical Case Story 1 (Extremities)Dokument0 SeitenPhysical Examination: Orthopedics: Clinical Case Story 1 (Extremities)Shamini ShanmugalingamNoch keine Bewertungen
- Case StudiesDokument4 SeitenCase StudiesSimran SukhijaNoch keine Bewertungen
- Introduction To Clinical Neurology: Acute Low Back and Neck PainDokument64 SeitenIntroduction To Clinical Neurology: Acute Low Back and Neck PainKhan A RehNoch keine Bewertungen
- Case ClinicalDokument6 SeitenCase ClinicalPerla Esmeralda Rangel RiveraNoch keine Bewertungen
- Soap Note Sub-Acute TkaDokument6 SeitenSoap Note Sub-Acute Tkaapi-3719716000% (1)
- Case Study 3 - Knee PainDokument12 SeitenCase Study 3 - Knee PainElizabeth Ho100% (9)
- Week 9 PCP Workbook QsDokument6 SeitenWeek 9 PCP Workbook Qsapi-479849199Noch keine Bewertungen
- Low Back Pain Lapkas 2Dokument27 SeitenLow Back Pain Lapkas 2rini najoanNoch keine Bewertungen
- HW4A SpineDokument3 SeitenHW4A SpineMary StrangeNoch keine Bewertungen
- Cauda Equina Syndrome Secondary To Lumbar Disc Herniation. Report of Three CasesDokument6 SeitenCauda Equina Syndrome Secondary To Lumbar Disc Herniation. Report of Three CasesSugi WilliamNoch keine Bewertungen
- Pleno Pemicu 2 Modul Muskuloskeletal Oleh: Kelompok Diskusi 5Dokument49 SeitenPleno Pemicu 2 Modul Muskuloskeletal Oleh: Kelompok Diskusi 5Ade Cahyo IslamiNoch keine Bewertungen
- Correct Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsVon EverandCorrect Your Pelvis and Heal your Back-Pain: The Self-Help Manual for Alleviating Back-Pain and other Musculo-Skeletal Aches and PainsNoch keine Bewertungen
- Peroneal Nerve Palsy Following Acp TreatmentDokument3 SeitenPeroneal Nerve Palsy Following Acp TreatmentLydwiNa JcNoch keine Bewertungen
- Wardha PresentationDokument141 SeitenWardha PresentationSatyendra OjhaNoch keine Bewertungen
- KTM Canada Weekly Race ReportDokument3 SeitenKTM Canada Weekly Race Reportapi-26009013Noch keine Bewertungen
- UntitledDokument4 SeitenUntitledDedy W. HerdiyantoNoch keine Bewertungen
- WP - Beginnings of Serbian Sokolism in HerzegovinaDokument19 SeitenWP - Beginnings of Serbian Sokolism in HerzegovinaMila VukNoch keine Bewertungen
- Joe Lewis ATTU 2012-10 PDFDokument3 SeitenJoe Lewis ATTU 2012-10 PDFBudo MediaNoch keine Bewertungen
- UntitledDokument30 SeitenUntitledIsabella KingsNoch keine Bewertungen
- Choral Speaking Script 2013Dokument4 SeitenChoral Speaking Script 2013Sakila Devi VenkitasamyNoch keine Bewertungen
- Famous InequalitiesDokument29 SeitenFamous InequalitiesG100% (2)
- KARATE-Compressed ListingDokument5 SeitenKARATE-Compressed Listingburtboyer_moyo928Noch keine Bewertungen
- Jet ForceDokument43 SeitenJet ForcePanteley Panov ProNoch keine Bewertungen
- A List of Codewords From Book 1 - The War-Torn KingdomDokument1 SeiteA List of Codewords From Book 1 - The War-Torn KingdomJoan FortunaNoch keine Bewertungen
- Granblue Fantasy - Wikipedia PDFDokument32 SeitenGranblue Fantasy - Wikipedia PDFRichard R.IgnacioNoch keine Bewertungen
- 183 PDFDokument116 Seiten183 PDFcalciumblessingNoch keine Bewertungen
- Ejercicios 3er CondicionalDokument5 SeitenEjercicios 3er CondicionalCUCOCUCOSNoch keine Bewertungen
- 2006 Nissan Sentra 1.8L 4 Cil (Qg18De) : Engine RestraintsDokument2 Seiten2006 Nissan Sentra 1.8L 4 Cil (Qg18De) : Engine Restraintsjimmy diaz tafurNoch keine Bewertungen
- Descargar PESDokument3 SeitenDescargar PESAlter PapuyNoch keine Bewertungen
- EXTM3UDokument6 SeitenEXTM3UTambah NilaiNoch keine Bewertungen
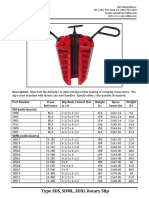
- Type SDS SDML SDXL Rotary Slip Cut SheetDokument2 SeitenType SDS SDML SDXL Rotary Slip Cut SheetJose Barrero100% (1)
- Flyers 2 Answer KeyDokument14 SeitenFlyers 2 Answer KeyhuynhlinNoch keine Bewertungen
- New Berlin EisenhowerDokument1 SeiteNew Berlin EisenhowerMyCommunityNOWNoch keine Bewertungen
- Body System 2º EnriqueDokument9 SeitenBody System 2º EnriqueRUIZ CANO EnriqueNoch keine Bewertungen
- Tilt Steering Column ComponentsDokument2 SeitenTilt Steering Column ComponentsjuanNoch keine Bewertungen
- Learn How To Type Faster. 20 Touch Typing Tips and Techniques - RatatypeDokument2 SeitenLearn How To Type Faster. 20 Touch Typing Tips and Techniques - RatatypeVictor JosephNoch keine Bewertungen
- Apple Will Have Its Presence at WWDC 2024Dokument3 SeitenApple Will Have Its Presence at WWDC 2024sumalesh.it22Noch keine Bewertungen
- King+of+Glory-Todd+Dulaney-Your+Great+Name.E 1Dokument3 SeitenKing+of+Glory-Todd+Dulaney-Your+Great+Name.E 1mcmeroNoch keine Bewertungen
- AI-Lecture 6 (Adversarial Search)Dokument68 SeitenAI-Lecture 6 (Adversarial Search)Braga Gladys MaeNoch keine Bewertungen
- Modifying .223 Magazines For The SAR-3Dokument13 SeitenModifying .223 Magazines For The SAR-3Arkane1988100% (1)
- Hoshigami - Hero Set EquipmentDokument9 SeitenHoshigami - Hero Set EquipmentEduardoBugsNoch keine Bewertungen
- Building Homebrew Pinball MachinesDokument20 SeitenBuilding Homebrew Pinball MachinesScott Danesi100% (1)
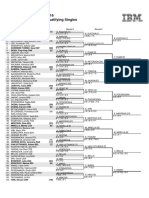
- US Open 2016 Women's Qualifying Singles: Round 1 Round 2 Round 3Dokument2 SeitenUS Open 2016 Women's Qualifying Singles: Round 1 Round 2 Round 3radiohtcNoch keine Bewertungen