Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Starbucks and Free TradeDokument9 SeitenStarbucks and Free TradeSandraPauwelsNoch keine Bewertungen
- Answers To Case Application Ch1-8Dokument13 SeitenAnswers To Case Application Ch1-8553601750% (2)
- Human BehaviorDokument14 SeitenHuman BehaviorJay Ann AguilarNoch keine Bewertungen
- Gas Leakage Detection Using Arm7 and ZigbeeDokument18 SeitenGas Leakage Detection Using Arm7 and ZigbeevinjamurisivaNoch keine Bewertungen
- POL 203 Intro To Western Political PhilosophyDokument202 SeitenPOL 203 Intro To Western Political PhilosophyShan Ali Shah100% (1)
- 2009 S+S BrochureDokument45 Seiten2009 S+S BrochureSMITH+SMITHNoch keine Bewertungen
- Midas Manual PDFDokument49 SeitenMidas Manual PDFNishad Kulkarni100% (1)
- 05 AccelerationDownIncline-2Dokument4 Seiten05 AccelerationDownIncline-2PeterNoch keine Bewertungen
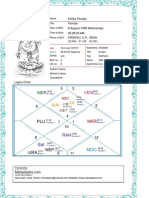
- Kritika Pandey (Kaushambi)Dokument15 SeitenKritika Pandey (Kaushambi)nishink9Noch keine Bewertungen
- Manual HDCVI DVR SeriesDokument144 SeitenManual HDCVI DVR SerieshansturNoch keine Bewertungen
- Engaging MathematicsDokument48 SeitenEngaging MathematicsDani ChiriacNoch keine Bewertungen
- Tilt-Up Building Seismic Design - Precast or Cast-In PlaceDokument3 SeitenTilt-Up Building Seismic Design - Precast or Cast-In PlacealexitomichaelNoch keine Bewertungen
- History of AAMI BIT StoryDokument11 SeitenHistory of AAMI BIT StoryManojNoch keine Bewertungen
- Bonus, Alexander Evan - The Metronomic Performance Practice - A History of Rhythm, Metronomes, and The Mechanization of MusicalityDokument597 SeitenBonus, Alexander Evan - The Metronomic Performance Practice - A History of Rhythm, Metronomes, and The Mechanization of MusicalityNoMoPoMo576100% (2)
- Technostream PDFDokument15 SeitenTechnostream PDFraulkmainaNoch keine Bewertungen
- Recruitment and Selection Process in Bangladesh Civil ServiceDokument9 SeitenRecruitment and Selection Process in Bangladesh Civil ServiceAllen AlfredNoch keine Bewertungen
- Sample of Interview Protocol - Questions Adopted From Timmons 1994Dokument2 SeitenSample of Interview Protocol - Questions Adopted From Timmons 1994Ash RafNoch keine Bewertungen
- Learning Centered AssDokument4 SeitenLearning Centered AssNica Rowena Bacani CajimatNoch keine Bewertungen
- CV Europass 20190114 LucianConstantin enDokument2 SeitenCV Europass 20190114 LucianConstantin enLucian DumitracheNoch keine Bewertungen
- Western Underground - HV and Ehv Cables-CmeDokument38 SeitenWestern Underground - HV and Ehv Cables-CmeA. Hassan100% (2)
- Certifi Cati N: Salary DoesDokument8 SeitenCertifi Cati N: Salary DoesGeeNoch keine Bewertungen
- The Ethics of Consumer Protection & Marketing: Ecture YnopsisDokument6 SeitenThe Ethics of Consumer Protection & Marketing: Ecture Ynopsiskuashask2Noch keine Bewertungen
- Prelims Coe Elec2Dokument72 SeitenPrelims Coe Elec2Sheena SapuayNoch keine Bewertungen
- 505xt 1 en PDFDokument242 Seiten505xt 1 en PDFSyed Mohammad NaveedNoch keine Bewertungen
- Grade 10 Unit 3 Task 4 Power Point DNADokument2 SeitenGrade 10 Unit 3 Task 4 Power Point DNAMohdFahdelNoch keine Bewertungen
- Dissolving Clouds With Your MindDokument14 SeitenDissolving Clouds With Your MindTamajong Tamajong PhilipNoch keine Bewertungen
- Full Download Strategic Management Text and Cases 9th Edition Dess Test BankDokument35 SeitenFull Download Strategic Management Text and Cases 9th Edition Dess Test Banksaumvirgen2375812100% (28)
- 9348 26140 1 PBDokument8 Seiten9348 26140 1 PBALIS TEBALNoch keine Bewertungen
- Chapter 2: Writing Process Writing Is A Process Which Involves Four Steps: - Planning - Drafting - Revising - Editing & ProofreadingDokument11 SeitenChapter 2: Writing Process Writing Is A Process Which Involves Four Steps: - Planning - Drafting - Revising - Editing & ProofreadingStein Bright Lateavi LawsonNoch keine Bewertungen
- C-Code Software Routines For Using The SPI Interface On The MAX7456 On-Screen DisplayDokument9 SeitenC-Code Software Routines For Using The SPI Interface On The MAX7456 On-Screen DisplayVinay Ashwath100% (2)