Das könnte Ihnen auch gefallen
- The Brigham Intensive Review of Internal Medicine Q&A Companion, 2eDokument227 SeitenThe Brigham Intensive Review of Internal Medicine Q&A Companion, 2eMalueth Angui100% (4)
- Cerebral Palsy Assessment ImportantDokument7 SeitenCerebral Palsy Assessment Importantabra_arr100% (2)
- PHARM ATI ReviewDokument76 SeitenPHARM ATI Reviewth233100% (1)
- Motivation, Compliance and Satisfaction in Orthodontic TreatmentDokument16 SeitenMotivation, Compliance and Satisfaction in Orthodontic TreatmentAkram AlsharaeeNoch keine Bewertungen
- Blood Bank ChecklistDokument4 SeitenBlood Bank ChecklistFIAZ MAQBOOL FAZILINoch keine Bewertungen
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDokument94 Seiten861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosNoch keine Bewertungen
- Litrature & Case StudyDokument74 SeitenLitrature & Case Studynaol buloNoch keine Bewertungen
- Review of Literature on Rabies Prevention and ControlDokument24 SeitenReview of Literature on Rabies Prevention and ControlBeah Claudette AbundoNoch keine Bewertungen
- 2014 Final Paediatric Exam (تم الحفظ تلقائيًا)Dokument258 Seiten2014 Final Paediatric Exam (تم الحفظ تلقائيًا)wea xcz100% (4)
- Sample Article CritiqueDokument7 SeitenSample Article CritiquerebeccaNoch keine Bewertungen
- 2022 Book AntimicrobialResistanceDokument606 Seiten2022 Book AntimicrobialResistanceFety Andriani100% (1)
- Dental Anxiety QuestionnairesDokument4 SeitenDental Anxiety QuestionnairesAmar BhochhibhoyaNoch keine Bewertungen
- Allen 12 02Dokument4 SeitenAllen 12 02Sarah_Zeitoun_792Noch keine Bewertungen
- Patients Compliance On Removable OrthodoDokument5 SeitenPatients Compliance On Removable OrthodoHasna HumairaNoch keine Bewertungen
- Factors Affecting Children's Adherence To Regular Dental AttendanceDokument12 SeitenFactors Affecting Children's Adherence To Regular Dental AttendanceDuanne EdvirgeNoch keine Bewertungen
- Jcs 8 105Dokument6 SeitenJcs 8 105nadia syestiNoch keine Bewertungen
- Linking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Dokument6 SeitenLinking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Catalina VenegasNoch keine Bewertungen
- Knowledge, Attitude and Practice of Tooth Wear Among Adults in Bertam, PenangDokument9 SeitenKnowledge, Attitude and Practice of Tooth Wear Among Adults in Bertam, PenangAlejandra AguilarNoch keine Bewertungen
- MI Gao2014Dokument12 SeitenMI Gao2014Xinyue XuNoch keine Bewertungen
- 2002 Dutch CI - SiDokument4 Seiten2002 Dutch CI - SiFreddy Campos SotoNoch keine Bewertungen
- Reasons For Use and Non-Use of Dental Services Among People Visiting A Dental College Hospital in India: A Descriptive Cross-Sectional StudyDokument6 SeitenReasons For Use and Non-Use of Dental Services Among People Visiting A Dental College Hospital in India: A Descriptive Cross-Sectional StudyRachmawati Dian PuspitasariNoch keine Bewertungen
- Satisfaction With Dental Appearance and Desired Esthetic Treatment in Saudi Dental PatientsDokument5 SeitenSatisfaction With Dental Appearance and Desired Esthetic Treatment in Saudi Dental PatientsSARA BUARISHNoch keine Bewertungen
- A Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsDokument5 SeitenA Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsazizahNoch keine Bewertungen
- Periodontal Referral Patterns of General Dentists: Lessons For Dental EducationDokument12 SeitenPeriodontal Referral Patterns of General Dentists: Lessons For Dental EducationVio VisanNoch keine Bewertungen
- Dental Health Status and Oral Health Behavior Among University Students From Five ASEAN CountriesDokument11 SeitenDental Health Status and Oral Health Behavior Among University Students From Five ASEAN CountriesAamirNoch keine Bewertungen
- Seale 2008Dokument5 SeitenSeale 2008PhanQuangHuyNoch keine Bewertungen
- Views on smoking cessation counselingDokument8 SeitenViews on smoking cessation counselingGurpinder TungNoch keine Bewertungen
- Jurnal AntibiotikDokument5 SeitenJurnal AntibiotikSela PutrianaNoch keine Bewertungen
- Update On Electronic Dental Record and Clinical Computing Adoption Among Dental Practices in The United StatesDokument16 SeitenUpdate On Electronic Dental Record and Clinical Computing Adoption Among Dental Practices in The United StatesNaji Z. ArandiNoch keine Bewertungen
- Validity Two Methods For Assessing Oral Health Status of PopulationsDokument9 SeitenValidity Two Methods For Assessing Oral Health Status of PopulationsSyarifah HaizanNoch keine Bewertungen
- Assessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityDokument6 SeitenAssessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityAdvanced Research PublicationsNoch keine Bewertungen
- Hesitance StudyDokument20 SeitenHesitance StudydrpiyuporwalNoch keine Bewertungen
- Cunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyDokument21 SeitenCunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyMilton david Rios serratoNoch keine Bewertungen
- Attitudes of Dental and Pharmacy Students To Oral Health Behaviour at Jazan University, Kingdom of Saudi ArabiaDokument5 SeitenAttitudes of Dental and Pharmacy Students To Oral Health Behaviour at Jazan University, Kingdom of Saudi ArabiaazizahNoch keine Bewertungen
- Factors in Uencing Satisfaction With The Process of Orthodontic Treatment in Adult PatientsDokument9 SeitenFactors in Uencing Satisfaction With The Process of Orthodontic Treatment in Adult PatientsLikhitaNoch keine Bewertungen
- Scientific Articles: 1. Dalius Petrauskas, Janina Petkeviciene, Jurate Klumbiene, Jolanta SiudikieneDokument8 SeitenScientific Articles: 1. Dalius Petrauskas, Janina Petkeviciene, Jurate Klumbiene, Jolanta SiudikieneChandra Sekhar ThatimatlaNoch keine Bewertungen
- Assessment of Knowledge Attitude and Practice of Oral Habits Among Health Care ProfessionalsDokument8 SeitenAssessment of Knowledge Attitude and Practice of Oral Habits Among Health Care ProfessionalsKrishna KadamNoch keine Bewertungen
- Introducing Dental Local Anaesthesia Using A Standardized Cognitive Behavioural TechniqueDokument15 SeitenIntroducing Dental Local Anaesthesia Using A Standardized Cognitive Behavioural TechniqueBunga Erlita RosaliaNoch keine Bewertungen
- Nonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewDokument11 SeitenNonpharmacologic Intervention On The Prevention of Pain and Anxiety During Pediatric Dental Care: A Systematic ReviewJorge Luis Ramos MaqueraNoch keine Bewertungen
- Linking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Dokument5 SeitenLinking Research To Clinical Practice: Flossing or Alternative Interdental Aids?Ana CernaianuNoch keine Bewertungen
- Evaluating oral health KAP of dental and medical studentsDokument4 SeitenEvaluating oral health KAP of dental and medical studentsAamirNoch keine Bewertungen
- Personality Type of Pediatric Dentists - Comparative Analysis and Associated FactorssDokument10 SeitenPersonality Type of Pediatric Dentists - Comparative Analysis and Associated FactorssObu KavithaNoch keine Bewertungen
- ContentServer AspDokument9 SeitenContentServer AspDeborah Morales CaychoNoch keine Bewertungen
- Pharmacology Literature ReviewDokument7 SeitenPharmacology Literature Reviewapi-703336450Noch keine Bewertungen
- Allied Success: Making The Most of The Relationship Between The Doctor and The Lab TechnicianDokument8 SeitenAllied Success: Making The Most of The Relationship Between The Doctor and The Lab TechnicianDiaa Eldin SaadNoch keine Bewertungen
- Eslam I PourDokument9 SeitenEslam I PourzumyNoch keine Bewertungen
- CDH 4550barasuol05Dokument5 SeitenCDH 4550barasuol05Deepakrajkc DeepuNoch keine Bewertungen
- Humphris 2009Dokument8 SeitenHumphris 2009Anonymous 9KcGpvNoch keine Bewertungen
- Carranza 2020Dokument40 SeitenCarranza 2020Soo SoniNoch keine Bewertungen
- 903 1224 2 PBDokument12 Seiten903 1224 2 PBFatul Chelseakers ZhinZhaiNoch keine Bewertungen
- Attitudes Towards Tooth Replacement Among Patients in Southern IndiaDokument9 SeitenAttitudes Towards Tooth Replacement Among Patients in Southern Indiaumerjaved86Noch keine Bewertungen
- Children's Dental Anxiety in The United Kingdom in 2003: Nigel M. Nuttall, Angela Gilbert, John MorrisDokument4 SeitenChildren's Dental Anxiety in The United Kingdom in 2003: Nigel M. Nuttall, Angela Gilbert, John MorrislusidaniatiNoch keine Bewertungen
- EBMgt 1Dokument8 SeitenEBMgt 1Delelegn EmwodewNoch keine Bewertungen
- Attitudes Toward Patient Safety Standards in US Dental SchoolsDokument7 SeitenAttitudes Toward Patient Safety Standards in US Dental SchoolsEko Wahyu AgustinNoch keine Bewertungen
- Study DesignsDokument36 SeitenStudy Designsz6f9cw8vwvNoch keine Bewertungen
- Advancing Infection Control in Dental Care SettingDokument12 SeitenAdvancing Infection Control in Dental Care SettingEndang SetiowatiNoch keine Bewertungen
- DiscussionDokument3 SeitenDiscussionMominah MayamNoch keine Bewertungen
- Evidence-Based Dentistry What's NewDokument5 SeitenEvidence-Based Dentistry What's NewGanisht AzmiNoch keine Bewertungen
- Dentist-Patient Communication As Perceived by Patients in Riyadh, Saudi ArabiaDokument8 SeitenDentist-Patient Communication As Perceived by Patients in Riyadh, Saudi ArabiaNisa HassanNoch keine Bewertungen
- Archive of SIDDokument6 SeitenArchive of SIDBeuty SavitriNoch keine Bewertungen
- Dentists' knowledge and practice of treating patients on oral antithromboticsDokument4 SeitenDentists' knowledge and practice of treating patients on oral antithromboticsBagis Emre GulNoch keine Bewertungen
- JordanDokument6 SeitenJordanNaji Z. ArandiNoch keine Bewertungen
- 2017 - Alomari Et AlDokument18 Seiten2017 - Alomari Et AlazeemathmariyamNoch keine Bewertungen
- Healthy Teens Counseling ApproachDokument6 SeitenHealthy Teens Counseling ApproachDebbie CharlotteNoch keine Bewertungen
- Oral Care Literature ReviewDokument7 SeitenOral Care Literature Reviewafmzfsqopfanlw100% (1)
- Knowledge of European Orthodontic Postgraduate Students On BiostatisticsDokument7 SeitenKnowledge of European Orthodontic Postgraduate Students On BiostatisticshemaadriNoch keine Bewertungen
- Articulo 6 BathiaDokument6 SeitenArticulo 6 BathiaMaria Ximena Torres PovedaNoch keine Bewertungen
- Uoi 142 FDokument9 SeitenUoi 142 FbkprosthoNoch keine Bewertungen
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationVon EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNoch keine Bewertungen
- Blood and Tissue Coccidian GuideDokument40 SeitenBlood and Tissue Coccidian GuideMichael DawitNoch keine Bewertungen
- Comparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingDokument2 SeitenComparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingFathima Sheik KatherNoch keine Bewertungen
- How To Maintain Throat HygieneDokument9 SeitenHow To Maintain Throat Hygieneankita singhNoch keine Bewertungen
- US Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreDokument4 SeitenUS Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreWilmer Zambrano GuerreroNoch keine Bewertungen
- Position Paper On Teenage PregnancyDokument3 SeitenPosition Paper On Teenage PregnancyMark Anthony CabangonNoch keine Bewertungen
- Congestive Heart Failure, Pulmonary Edema, and CPAPDokument35 SeitenCongestive Heart Failure, Pulmonary Edema, and CPAPSherwan R Shal100% (1)
- Source Control in Emergency General SurgeryDokument21 SeitenSource Control in Emergency General SurgerylaviniaNoch keine Bewertungen
- Health Check Template FormDokument2 SeitenHealth Check Template Form백만호Noch keine Bewertungen
- Lesson 3 ReviewDokument4 SeitenLesson 3 ReviewHo Yong WaiNoch keine Bewertungen
- Health and IllnessDokument2 SeitenHealth and IllnessLize Decotelli HubnerNoch keine Bewertungen
- Minimum Inhibitory ConcentrationDokument7 SeitenMinimum Inhibitory ConcentrationToshio HamazakiNoch keine Bewertungen
- Recent Trends in Insulin Drug Delivery SystemDokument39 SeitenRecent Trends in Insulin Drug Delivery Systemandry natanel tonyNoch keine Bewertungen
- KenyaEMR v17.3.1 Release Notes SummaryDokument3 SeitenKenyaEMR v17.3.1 Release Notes SummaryMigori Art DataNoch keine Bewertungen
- Dental CatalogueDokument28 SeitenDental CataloguePaulus LagadanNoch keine Bewertungen
- Delusional Jealusy - FullDokument17 SeitenDelusional Jealusy - FullnicolasNoch keine Bewertungen
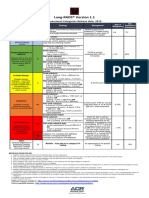
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokument1 SeiteLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNoch keine Bewertungen
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDokument8 SeitenVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengNoch keine Bewertungen
- Critical Thinking Case Study #18:: Sickle-Cell AnemiaDokument15 SeitenCritical Thinking Case Study #18:: Sickle-Cell AnemiaHakima Hadji DaudNoch keine Bewertungen
- QuestionsDokument6 SeitenQuestionsLorvic Andrew Juanson UmaliNoch keine Bewertungen
- Community Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsDokument4 SeitenCommunity Health and Program Services (CHAPS) : Health Disparities Among Racial/Ethnic PopulationsMuhammad Bachiar SafrudinNoch keine Bewertungen
- Sleep and The Risk of Chronic Kidney Disease: A Cohort StudyDokument8 SeitenSleep and The Risk of Chronic Kidney Disease: A Cohort StudyEtaursaeNoch keine Bewertungen