Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Literature and Skepticism (Pablo Oyarzun)Dokument232 SeitenLiterature and Skepticism (Pablo Oyarzun)Fernando MouraNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Modes of SpeciationDokument3 SeitenModes of SpeciationRichard Balicat Jr.Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Lesson Plan 1 ElaDokument12 SeitenLesson Plan 1 Elaapi-242017773Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Fanmade Translation Dramatis Personae II (By Blues and Aophis)Dokument50 SeitenFanmade Translation Dramatis Personae II (By Blues and Aophis)BulshockNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Criminalistic SDokument2 SeitenCriminalistic SEdmund HerceNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
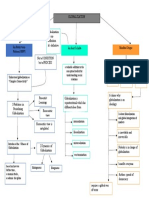
- GCWORLD Concept MapDokument1 SeiteGCWORLD Concept MapMoses Gabriel ValledorNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Mystery of NegationDokument5 SeitenMystery of NegationAbe Li HamzahNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Bias-Free LanguageDokument26 SeitenBias-Free LanguageFerdinand A. Ramos100% (1)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- How Google WorksDokument9 SeitenHow Google WorksHoangDuongNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Documented Essay About EmojisDokument8 SeitenDocumented Essay About EmojisSweet MulanNoch keine Bewertungen
- Daily Lesson Log Subject English Grade Level: 8 Grading Period: I. ObjectivesDokument2 SeitenDaily Lesson Log Subject English Grade Level: 8 Grading Period: I. ObjectivesArchelSayagoNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Toyota Forklift 02 5fg28!02!5fg30 Parts CatalogDokument22 SeitenToyota Forklift 02 5fg28!02!5fg30 Parts Catalognathanielsmith070288xgd100% (115)
- Ilhaam (Enlightenment) A Play by Manav Kaul: Scene - IDokument19 SeitenIlhaam (Enlightenment) A Play by Manav Kaul: Scene - IPrateek DwivediNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Traditional Public Administration Versus The New Public Management: Accountability Versus Efficiency James P. PfiffnerDokument10 SeitenTraditional Public Administration Versus The New Public Management: Accountability Versus Efficiency James P. PfiffnerChantal FoleriNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- ProspectingDokument21 SeitenProspectingCosmina Andreea ManeaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Where You Stand Determines What You SeeDokument6 SeitenWhere You Stand Determines What You SeeMylene Rochelle Manguiob Cruz100% (1)
- Trolldómr in Early Medieval Scandinavia-Catharina Raudvere PDFDokument50 SeitenTrolldómr in Early Medieval Scandinavia-Catharina Raudvere PDFludaisi100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- A Study of The Semiotics of Print AdvertisementsDokument42 SeitenA Study of The Semiotics of Print AdvertisementsMay100% (1)
- Conflict ManagementDokument12 SeitenConflict ManagementRaquel O. MendozaNoch keine Bewertungen
- CYP Case Study Assignment Virginia Toole 20260933 Dec 3, 2019 Part 2Dokument9 SeitenCYP Case Study Assignment Virginia Toole 20260933 Dec 3, 2019 Part 2Ginny Viccy C TNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Muhammad The Last Prophet in The Bible by Kais Al-KalbyDokument293 SeitenMuhammad The Last Prophet in The Bible by Kais Al-KalbyWaqarNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Ethical Decision Making and Ethical LeadershipDokument11 SeitenEthical Decision Making and Ethical LeadershipmisonotoNoch keine Bewertungen
- Voelz - Newton and Einstein at The Foot of The CrossDokument14 SeitenVoelz - Newton and Einstein at The Foot of The CrossEric W. RodgersNoch keine Bewertungen
- BRMM 575 Chapter 2Dokument5 SeitenBRMM 575 Chapter 2Moni TafechNoch keine Bewertungen
- Anticipating Strategy DecayDokument14 SeitenAnticipating Strategy DecayRoshela KhanNoch keine Bewertungen
- Idiomatic Expressions Module 1Dokument20 SeitenIdiomatic Expressions Module 1Jing ReginaldoNoch keine Bewertungen
- College of St. John - Roxas: ACTIVITY SHEETS (WEEK 2-Methods of Philosophizing)Dokument3 SeitenCollege of St. John - Roxas: ACTIVITY SHEETS (WEEK 2-Methods of Philosophizing)Lalaine LuzaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Adventist Movement Its Relationship To The Seventh Day Church of God PDFDokument54 SeitenThe Adventist Movement Its Relationship To The Seventh Day Church of God PDFCraig MartinNoch keine Bewertungen
- Lecture 20 RobocupDokument17 SeitenLecture 20 RobocupKartika MunirNoch keine Bewertungen
- BROSUR 58th TEFLIN Conference 2g38ungDokument3 SeitenBROSUR 58th TEFLIN Conference 2g38ungAngela IndrianiNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)