Das könnte Ihnen auch gefallen
- Patient Studies in Valvular, Congenital, and Rarer Forms of Cardiovascular Disease: An Integrative ApproachVon EverandPatient Studies in Valvular, Congenital, and Rarer Forms of Cardiovascular Disease: An Integrative ApproachNoch keine Bewertungen
- CPAP SlidesDokument52 SeitenCPAP SlidesAnusha Verghese100% (1)
- Case Presentation On Pediatric Anesthesia For Thoracotomy andDokument16 SeitenCase Presentation On Pediatric Anesthesia For Thoracotomy andHenoke MuluNoch keine Bewertungen
- Final Common Medical Surgical EmergenciesDokument99 SeitenFinal Common Medical Surgical Emergenciesapi-195799092Noch keine Bewertungen
- Pulmonary Hypertension in The CICUDokument50 SeitenPulmonary Hypertension in The CICUCardiacCareCenterMCHNoch keine Bewertungen
- Subcutaneous EmphysemaDokument95 SeitenSubcutaneous EmphysemaRaina AbadNoch keine Bewertungen
- Choking in ChildrenDokument32 SeitenChoking in ChildrenDarari GenaditaNoch keine Bewertungen
- Intra-Operative PEEP Vs ZEEPDokument37 SeitenIntra-Operative PEEP Vs ZEEPMohamed RifanNoch keine Bewertungen
- Bilateral Secondary Spontaneous PneumothoraxDokument27 SeitenBilateral Secondary Spontaneous Pneumothoraxgaddam venkata mohanNoch keine Bewertungen
- Case PPOK-Dr Riki TenggaraDokument38 SeitenCase PPOK-Dr Riki Tenggarabudi_26690Noch keine Bewertungen
- MoonlightingDokument282 SeitenMoonlightingMeg Mateo100% (1)
- Case Presentation On Management of Abdomenal Injury (2) - 2Dokument83 SeitenCase Presentation On Management of Abdomenal Injury (2) - 2tadeleNoch keine Bewertungen
- Pediatric Surgery Dr. A. IgamaDokument6 SeitenPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNoch keine Bewertungen
- Yuniarti, CHF, Krisis Tiroid, CAP Duty HannaDokument17 SeitenYuniarti, CHF, Krisis Tiroid, CAP Duty HannaHanna GustinNoch keine Bewertungen
- Anaesthesia For Burns: Dr. Alex Kan Senior Consultant Dept of Anaesthesia & SICU Singapore General HospitalDokument46 SeitenAnaesthesia For Burns: Dr. Alex Kan Senior Consultant Dept of Anaesthesia & SICU Singapore General HospitalTaufik Akbar Faried LubisNoch keine Bewertungen
- In-Service Exam Review 2009 Emergency MedicineDokument147 SeitenIn-Service Exam Review 2009 Emergency Medicineiamo107501100% (1)
- Acute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarDokument47 SeitenAcute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarAsri PrameswariNoch keine Bewertungen
- Pneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahaDokument50 SeitenPneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahappgpcsNoch keine Bewertungen
- Bronchial HygieneDokument37 SeitenBronchial HygieneRayan MohhamadNoch keine Bewertungen
- Case Presentation ETD (COPD)Dokument45 SeitenCase Presentation ETD (COPD)Dzachary13Noch keine Bewertungen
- Edendale GuidelinesDokument44 SeitenEdendale GuidelinesBem Fakultas Kedokteran UnlamNoch keine Bewertungen
- Neardrowning: Prehospital and Emergency Department ManagementDokument34 SeitenNeardrowning: Prehospital and Emergency Department ManagementAyeNoch keine Bewertungen
- Neonatal PneumoniaDokument29 SeitenNeonatal PneumoniaChristian JaraNoch keine Bewertungen
- Cough, Dyspnoea: DR - Veena 2016 - 2017Dokument109 SeitenCough, Dyspnoea: DR - Veena 2016 - 2017HanisahNoch keine Bewertungen
- Critical Incidentsduring Perioperative Period Sept 2011Dokument106 SeitenCritical Incidentsduring Perioperative Period Sept 2011wellawalalasithNoch keine Bewertungen
- Prezentare Caz Clinic Ventilatia Mecanica IntraoperatorieDokument55 SeitenPrezentare Caz Clinic Ventilatia Mecanica Intraoperatorieralucaioana89Noch keine Bewertungen
- Heri Sunoto, CKD CHF, Duty HannaDokument17 SeitenHeri Sunoto, CKD CHF, Duty HannaHanna GustinNoch keine Bewertungen
- CPDDokument78 SeitenCPDEira Rajkumar50% (2)
- Approach To Cough: Mark Angelo Z. Ponferrado, MD Pre-ResidentDokument32 SeitenApproach To Cough: Mark Angelo Z. Ponferrado, MD Pre-ResidentMark Angelo PonferradoNoch keine Bewertungen
- Difficult Cases Septic ShockDokument53 SeitenDifficult Cases Septic ShockHoa Cỏ ĐậuNoch keine Bewertungen
- Acute Abdominal PainDokument59 SeitenAcute Abdominal PainanuchitjitsangNoch keine Bewertungen
- Diffus Peritonitis 5-8-2015Dokument11 SeitenDiffus Peritonitis 5-8-2015Vanny OcktariaNoch keine Bewertungen
- Mechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDDokument25 SeitenMechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDsarevNoch keine Bewertungen
- DR Fiona Dignan - Acute Haematological EmergenciesDokument37 SeitenDR Fiona Dignan - Acute Haematological EmergenciesAndreKrisleeNoch keine Bewertungen
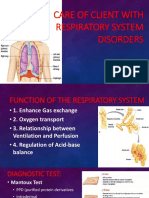
- Care of Client With Respiratory System DisordersDokument17 SeitenCare of Client With Respiratory System DisordersAYTONA, JAMAICA F.Noch keine Bewertungen
- Pre and Post Op Management of Surgical PatientsDokument36 SeitenPre and Post Op Management of Surgical PatientsPrabhakar KumarNoch keine Bewertungen
- Nursing TerminologyDokument48 SeitenNursing Terminologyyuhuma_qyu68410% (1)
- Case Presentation HypokalemiaDokument32 SeitenCase Presentation HypokalemiaFrances Bituin100% (1)
- Pedia BAIEDokument49 SeitenPedia BAIEDarlene Clarice V. LabacladoNoch keine Bewertungen
- 1 Early Management of Trauma Patient in The HospitalDokument23 Seiten1 Early Management of Trauma Patient in The HospitalkgnmatinNoch keine Bewertungen
- Aril PneumothoraxDokument11 SeitenAril PneumothoraxyongkyNoch keine Bewertungen
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDokument49 SeitenShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- Gastrointestinal Disorders: CPT Donald C Palma MCDokument28 SeitenGastrointestinal Disorders: CPT Donald C Palma MCJorge RabajaNoch keine Bewertungen
- Tria O Kolelithiasis 12 Maret 18Dokument11 SeitenTria O Kolelithiasis 12 Maret 18annanurina2Noch keine Bewertungen
- Managing Crashing Patients in The FieldDokument73 SeitenManaging Crashing Patients in The FieldWilliam L McGill100% (2)
- Pneumonia and CXR Revision: Leigh-Anne HillDokument51 SeitenPneumonia and CXR Revision: Leigh-Anne Hillapi-195799092Noch keine Bewertungen
- Muhammad Nur, Penkes Ec SAE DD Hypoxia, Duty HannaDokument16 SeitenMuhammad Nur, Penkes Ec SAE DD Hypoxia, Duty HannaHanna GustinNoch keine Bewertungen
- Nurhayati, Female, 61 Yo, Neurology Ward: Chief Complaint: Present Illness HistoryDokument26 SeitenNurhayati, Female, 61 Yo, Neurology Ward: Chief Complaint: Present Illness Historyannisa edwarNoch keine Bewertungen
- LAPJAG DR RidwanDokument13 SeitenLAPJAG DR RidwanElsy Pramitha SariNoch keine Bewertungen
- Clinic PresentationDokument30 SeitenClinic PresentationHein Phyo WaiNoch keine Bewertungen
- Perforated Peptic Ulcer - An UpdateDokument17 SeitenPerforated Peptic Ulcer - An UpdateRama_Aditya_KNoch keine Bewertungen
- Respiratory EmergencyDokument36 SeitenRespiratory EmergencyHtet Htet LinNoch keine Bewertungen
- Grand ReportsDokument60 SeitenGrand ReportsfilchibuffNoch keine Bewertungen
- 11b - Sepsis Case Studies - Randy WaxDokument25 Seiten11b - Sepsis Case Studies - Randy WaxSukma EffendyNoch keine Bewertungen
- Necrotizing Enterocolitis: Reproduction System 2010Dokument39 SeitenNecrotizing Enterocolitis: Reproduction System 2010Anonymous Af24L7Noch keine Bewertungen
- Mechanical Ventilation Handout - AllenhoDokument22 SeitenMechanical Ventilation Handout - Allenhofriyaz8197100% (1)
- Duty Report - Rosni (DR - Gari)Dokument9 SeitenDuty Report - Rosni (DR - Gari)RudiErwinKurniawanNoch keine Bewertungen
- Duty Report - Rosni (DR - Gari)Dokument9 SeitenDuty Report - Rosni (DR - Gari)RudiErwinKurniawanNoch keine Bewertungen
- 58f6anesthesia For Laparoscopic SurgeriesDokument56 Seiten58f6anesthesia For Laparoscopic SurgeriesSayed NourNoch keine Bewertungen
- Armaniar Leukemia AkutDokument13 SeitenArmaniar Leukemia AkutJongga SiahaanNoch keine Bewertungen
- CebuanoDokument1 SeiteCebuanoanon_58478535150% (2)
- Unit 3 RequirementsDokument4 SeitenUnit 3 Requirementsravioli kimNoch keine Bewertungen
- Duterte Vs SandiganbayanDokument17 SeitenDuterte Vs SandiganbayanAnonymous KvztB3Noch keine Bewertungen
- Describe The Forms of Agency CompensationDokument2 SeitenDescribe The Forms of Agency CompensationFizza HassanNoch keine Bewertungen
- Spice Processing UnitDokument3 SeitenSpice Processing UnitKSHETRIMAYUM MONIKA DEVINoch keine Bewertungen
- Sheet PilesDokument5 SeitenSheet PilesolcayuzNoch keine Bewertungen
- Rajasekhara Dasa - Guide To VrindavanaDokument35 SeitenRajasekhara Dasa - Guide To VrindavanaDharani DharendraNoch keine Bewertungen
- Anxxx PDFDokument13 SeitenAnxxx PDFDamion HaleNoch keine Bewertungen
- Book Review On PandeymoniumDokument2 SeitenBook Review On PandeymoniumJanhavi ThakkerNoch keine Bewertungen
- PsychometricsDokument4 SeitenPsychometricsCor Villanueva33% (3)
- Financial Performance Report General Tyres and Rubber Company-FinalDokument29 SeitenFinancial Performance Report General Tyres and Rubber Company-FinalKabeer QureshiNoch keine Bewertungen
- Land Building and MachineryDokument26 SeitenLand Building and MachineryNathalie Getino100% (1)
- MEAL DPro Guide - EnglishDokument145 SeitenMEAL DPro Guide - EnglishkatlehoNoch keine Bewertungen
- Imc Case - Group 3Dokument5 SeitenImc Case - Group 3Shubham Jakhmola100% (3)
- Boot CommandDokument40 SeitenBoot CommandJimmywang 王修德Noch keine Bewertungen
- Queen of Hearts Rules - FinalDokument3 SeitenQueen of Hearts Rules - FinalAudrey ErwinNoch keine Bewertungen
- Novedades Jaltest CV en 887Dokument14 SeitenNovedades Jaltest CV en 887Bruce LyndeNoch keine Bewertungen
- Meditation For AddictionDokument2 SeitenMeditation For AddictionharryNoch keine Bewertungen
- Simplified Electronic Design of The Function : ARMTH Start & Stop SystemDokument6 SeitenSimplified Electronic Design of The Function : ARMTH Start & Stop SystembadrNoch keine Bewertungen
- SRL CompressorsDokument20 SeitenSRL Compressorssthe03Noch keine Bewertungen
- OptiX OSN 8800 6800 3800 Configuration Guide (V100R007)Dokument924 SeitenOptiX OSN 8800 6800 3800 Configuration Guide (V100R007)vladNoch keine Bewertungen
- Executive SummaryDokument3 SeitenExecutive SummarySofia ArissaNoch keine Bewertungen
- 30rap 8pd PDFDokument76 Seiten30rap 8pd PDFmaquinagmcNoch keine Bewertungen
- Picc Lite ManualDokument366 SeitenPicc Lite Manualtanny_03Noch keine Bewertungen
- Astm D1895 17Dokument4 SeitenAstm D1895 17Sonia Goncalves100% (1)
- Kumar-2011-In Vitro Plant Propagation A ReviewDokument13 SeitenKumar-2011-In Vitro Plant Propagation A ReviewJuanmanuelNoch keine Bewertungen
- The Nature of Mathematics: "Nature's Great Books Is Written in Mathematics" Galileo GalileiDokument9 SeitenThe Nature of Mathematics: "Nature's Great Books Is Written in Mathematics" Galileo GalileiLei-Angelika TungpalanNoch keine Bewertungen
- Phylogenetic Tree: GlossaryDokument7 SeitenPhylogenetic Tree: GlossarySab ka bada FanNoch keine Bewertungen
- Supply Chain Management: A Framework of Understanding D. Du Toit & P.J. VlokDokument14 SeitenSupply Chain Management: A Framework of Understanding D. Du Toit & P.J. VlokchandanaNoch keine Bewertungen
- Marriot CaseDokument15 SeitenMarriot CaseArsh00100% (7)