Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 4TH Quarter Test Grade 7Dokument3 Seiten4TH Quarter Test Grade 7Nhey Cawigan92% (13)
- Classical Asian Herbal TherapyDokument116 SeitenClassical Asian Herbal TherapylinecurNoch keine Bewertungen
- English-Italian Medical GlossaryDokument18 SeitenEnglish-Italian Medical GlossaryAnnalisa DassistiNoch keine Bewertungen
- Neurological SystemDokument7 SeitenNeurological SystemDaintyGarcia100% (1)
- Stroke Assessment and Prevention Pocket CardsDokument19 SeitenStroke Assessment and Prevention Pocket CardsFilipa FigueiredoNoch keine Bewertungen
- 2007 Engleza Heart FailureDokument38 Seiten2007 Engleza Heart FailureDanielaNoch keine Bewertungen
- Dislipidemii Vlad 2011Dokument40 SeitenDislipidemii Vlad 2011DanielaNoch keine Bewertungen
- Pulmonary ThromboembolismDokument25 SeitenPulmonary ThromboembolismDanielaNoch keine Bewertungen
- Tromboza VenoasaDokument4 SeitenTromboza VenoasaDanielaNoch keine Bewertungen
- Urologic and Nephrologic DisordersDokument49 SeitenUrologic and Nephrologic DisordersDanielaNoch keine Bewertungen
- Early Diagnosis of NeoplasisDokument25 SeitenEarly Diagnosis of NeoplasisDanielaNoch keine Bewertungen
- 09 Acute Med AbdDokument42 Seiten09 Acute Med AbdDanielaNoch keine Bewertungen
- 12 AnaemiasDokument52 Seiten12 AnaemiasDanielaNoch keine Bewertungen
- 12 Hemorrhagic SyndromesDokument16 Seiten12 Hemorrhagic SyndromesDanielaNoch keine Bewertungen
- 10 Patient With Liver DiseaseDokument40 Seiten10 Patient With Liver DiseaseDanielaNoch keine Bewertungen
- 11 Gastrointestinal DiseasesDokument32 Seiten11 Gastrointestinal DiseasesDanielaNoch keine Bewertungen
- Argent in ADokument1 SeiteArgent in ADanielaNoch keine Bewertungen
- 05 Patient With Acute Thoracic PainDokument69 Seiten05 Patient With Acute Thoracic PainDanielaNoch keine Bewertungen
- 07 The Valvular PatientDokument83 Seiten07 The Valvular PatientDanielaNoch keine Bewertungen
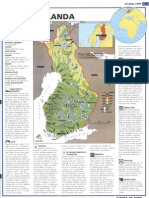
- Finland ADokument1 SeiteFinland AmamaluiraresNoch keine Bewertungen
- 04 Patient With HypertensionDokument47 Seiten04 Patient With HypertensionDanielaNoch keine Bewertungen
- The Patient With Fever: Assoc. Prof. Simona DraganDokument29 SeitenThe Patient With Fever: Assoc. Prof. Simona DraganDanielaNoch keine Bewertungen
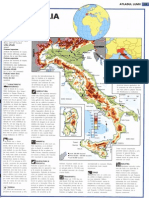
- It Ali ADokument1 SeiteIt Ali ADanielaNoch keine Bewertungen
- BraziliaDokument1 SeiteBraziliamamaluiraresNoch keine Bewertungen
- Treatment of CP With Chinese Scalp Acupuncture 17 June HaoDokument6 SeitenTreatment of CP With Chinese Scalp Acupuncture 17 June HaoSebastiano Serra100% (1)
- Headache History TakingDokument5 SeitenHeadache History TakingRao Rizwan ShakoorNoch keine Bewertungen
- Learning Objectives: Advanced Therapeutics StrokeDokument15 SeitenLearning Objectives: Advanced Therapeutics StrokeChetan PataliNoch keine Bewertungen
- BSN - 4C: PresentorsDokument52 SeitenBSN - 4C: PresentorsHanya Bint Potawan100% (1)
- Pocket Guide to Critical Care Pharmacotherapy, 2e SÁCH DỊCHDokument185 SeitenPocket Guide to Critical Care Pharmacotherapy, 2e SÁCH DỊCHHoàng LongNoch keine Bewertungen
- Angiographic Efficacy of The Atriclip Left Atrial Appendage Exclusion Device Placed by Minimally Invasive Thoracoscopic ApproachDokument10 SeitenAngiographic Efficacy of The Atriclip Left Atrial Appendage Exclusion Device Placed by Minimally Invasive Thoracoscopic ApproachdokterBramNoch keine Bewertungen
- Questioned DocsDokument5 SeitenQuestioned DocsSay DoradoNoch keine Bewertungen
- Chapter 026 CoagulationDokument7 SeitenChapter 026 Coagulationthubtendrolma100% (3)
- Diabetes and Cerebrovascular DiseaseDokument30 SeitenDiabetes and Cerebrovascular DiseaseAJVAZI100% (4)
- Pelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future PerspectivesDokument15 SeitenPelzer Et Al 2023 Neurological and Psychiatric Comorbidities of Migraine Concepts and Future Perspectivespaulo gutierrezNoch keine Bewertungen
- Kode Diagnosa PRBDokument9 SeitenKode Diagnosa PRBpuskesmas sobangNoch keine Bewertungen
- Drugs For Cardiovascular Diseases: May Florence D. Bacayo, Msc. May - Florence@Msu - Edu.MyDokument202 SeitenDrugs For Cardiovascular Diseases: May Florence D. Bacayo, Msc. May - Florence@Msu - Edu.MySubha ShankareeNoch keine Bewertungen
- NIH Public Access: The Risks Associated With Alcohol Use and AlcoholismDokument15 SeitenNIH Public Access: The Risks Associated With Alcohol Use and AlcoholismPritty ElenutzaNoch keine Bewertungen
- Synthesis PaperDokument5 SeitenSynthesis Paperapi-358143741Noch keine Bewertungen
- Differential Diagnosis of StrokeDokument2 SeitenDifferential Diagnosis of Strokeamna_badar1Noch keine Bewertungen
- Cardiovascular Disease: By: Bs Nutrition and Dietetics StudentsDokument13 SeitenCardiovascular Disease: By: Bs Nutrition and Dietetics StudentsMiles ViaNoch keine Bewertungen
- Broccoli Based MedicineDokument3 SeitenBroccoli Based MedicineMatthew StoneNoch keine Bewertungen
- FILE - 20191227 - 140801 - 4. Đề-thi-HKI-avcn K43Dokument8 SeitenFILE - 20191227 - 140801 - 4. Đề-thi-HKI-avcn K43Liễu PhươngNoch keine Bewertungen
- HyfrhDokument34 SeitenHyfrhmebibegNoch keine Bewertungen
- Characteristics of Ischaemic Stroke Associated With COVID-19Dokument3 SeitenCharacteristics of Ischaemic Stroke Associated With COVID-19Qisti AshariNoch keine Bewertungen
- Apostila R2Dokument469 SeitenApostila R2Lucas TheotonioNoch keine Bewertungen
- Modern Management of Hypertensive Emergencies: Review ArticleDokument8 SeitenModern Management of Hypertensive Emergencies: Review ArticleAnthony PonceNoch keine Bewertungen
- American Stroke AssociationDokument1 SeiteAmerican Stroke AssociationritadoloksaribuNoch keine Bewertungen
- Umbilical Cord Blood BankingDokument290 SeitenUmbilical Cord Blood BankingcmNoch keine Bewertungen
- Brief History of AerobicsDokument4 SeitenBrief History of Aerobicsshyne pabloNoch keine Bewertungen