Das könnte Ihnen auch gefallen
- The Art of PhacoemulsificationDokument544 SeitenThe Art of PhacoemulsificationDaniel Fernández Gajardo100% (3)
- Top of Page Patients and Methods Results Discussion Conclusion BibliographyDokument16 SeitenTop of Page Patients and Methods Results Discussion Conclusion BibliographyentsrmcNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesDokument9 Seiten(10920684 - Neurosurgical Focus) Surgical Management of Trigeminal Schwannomas - Defining The Role For Endoscopic Endonasal ApproachesasiyazaidiaNoch keine Bewertungen
- Endoscopic Discectomy by HooglandDokument8 SeitenEndoscopic Discectomy by HooglandKaustubh KeskarNoch keine Bewertungen
- 2-9 Reda KamelDokument8 Seiten2-9 Reda KamelMoustafa Amin AlyNoch keine Bewertungen
- Cers Cadwell LucDokument3 SeitenCers Cadwell LucVictorioStokNoch keine Bewertungen
- Inferior Alveolar Nerve Block Anesthesia Via The Retromolar Triangle, An Alternative For Patients With Blood DyscrasiasDokument5 SeitenInferior Alveolar Nerve Block Anesthesia Via The Retromolar Triangle, An Alternative For Patients With Blood DyscrasiasGina CastilloNoch keine Bewertungen
- Endoscopic Skull Base SurgeryDokument25 SeitenEndoscopic Skull Base Surgerypramod454992Noch keine Bewertungen
- (Journal of Neurosurgery) Neuroendoscopic Approach To Intraventricular LesionsDokument10 Seiten(Journal of Neurosurgery) Neuroendoscopic Approach To Intraventricular LesionsAniaNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Endoscopic Management of Intracranial CystsDokument9 Seiten(10920684 - Neurosurgical Focus) Endoscopic Management of Intracranial Cystsrifki irsyadNoch keine Bewertungen
- 05 CastelnuovoDokument7 Seiten05 Castelnuovogabriele1977Noch keine Bewertungen
- Expanded Endonasal Approach - The Rostrocaudal Axis Part I PDFDokument12 SeitenExpanded Endonasal Approach - The Rostrocaudal Axis Part I PDFIvonne PerezNoch keine Bewertungen
- Resultados de Cadwell Luc en CERS FallidaDokument3 SeitenResultados de Cadwell Luc en CERS FallidaVictorioStokNoch keine Bewertungen
- Endoscopic Dacryocystorhinostomy Seems Promising For Lacrimal StenosisDokument4 SeitenEndoscopic Dacryocystorhinostomy Seems Promising For Lacrimal StenosisAgitha Melita PutriNoch keine Bewertungen
- Original Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyDokument7 SeitenOriginal Article: 360 Degree Subannular Tympanoplasty: A Retrospective StudyAkanshaNoch keine Bewertungen
- Endoscopic Sinus Surgery: Indications and Complications: February 2020Dokument7 SeitenEndoscopic Sinus Surgery: Indications and Complications: February 2020husnul khatimahNoch keine Bewertungen
- Open SeptorhinoplastyDokument6 SeitenOpen SeptorhinoplastybarbiemeNoch keine Bewertungen
- Condilectomia Intra OralDokument7 SeitenCondilectomia Intra OralJuan Carlos MeloNoch keine Bewertungen
- Ceo 6 263Dokument3 SeitenCeo 6 263Yusa Has JulianaNoch keine Bewertungen
- The Management of Sinonasal Inverted Papilloma: Our ExperienceDokument7 SeitenThe Management of Sinonasal Inverted Papilloma: Our Experiencesri ayu lestari wulandariNoch keine Bewertungen
- Ann Burns and Fire Disasters 29 209Dokument6 SeitenAnn Burns and Fire Disasters 29 209fabian hernandez medinaNoch keine Bewertungen
- 05 04 06 Cerebrospinal Fluid RhinorrheaDokument53 Seiten05 04 06 Cerebrospinal Fluid RhinorrheaiachapraNoch keine Bewertungen
- Transcanal Endoscopic Ear Surgery For Middle Ear Cholesteatoma in Journal Club 07.5.18Dokument5 SeitenTranscanal Endoscopic Ear Surgery For Middle Ear Cholesteatoma in Journal Club 07.5.18Abdur RahmanNoch keine Bewertungen
- Electrocautery Versus Curette Adenoidectomy: Comparison of Postoperative ResultsDokument8 SeitenElectrocautery Versus Curette Adenoidectomy: Comparison of Postoperative Resultsthanhb1lqdNoch keine Bewertungen
- Temporal Bone Encephalocele and Cerebrospinal Fluid FistulaDokument9 SeitenTemporal Bone Encephalocele and Cerebrospinal Fluid FistulaSa'Deu FondjoNoch keine Bewertungen
- Computed Tomographic Evaluation of Anatomical Variations of Paranasal Sinus RegionDokument5 SeitenComputed Tomographic Evaluation of Anatomical Variations of Paranasal Sinus RegionConstantin StanNoch keine Bewertungen
- Inferior Turbinectomy For Nasal Obstruction Review of 75 CasesDokument4 SeitenInferior Turbinectomy For Nasal Obstruction Review of 75 CasesMeilina Elin WardhaniNoch keine Bewertungen
- Retrosigmoid Intradural Suprameatal Approach To Meckel's Cave and The Middle Fossa Surgical Technique and Outcome, Tatagiba, 2000Dokument7 SeitenRetrosigmoid Intradural Suprameatal Approach To Meckel's Cave and The Middle Fossa Surgical Technique and Outcome, Tatagiba, 2000CAMILO ARMANDO BENAVIDES BURBANONoch keine Bewertungen
- International Journal of Surgery Case ReportsDokument5 SeitenInternational Journal of Surgery Case Reportscarlos javier andraadeNoch keine Bewertungen
- Original ArticleDokument9 SeitenOriginal ArticleJason HuangNoch keine Bewertungen
- Ir 2867Dokument8 SeitenIr 2867shamsshanti999Noch keine Bewertungen
- Sanai 2010Dokument7 SeitenSanai 2010Diane MxNoch keine Bewertungen
- Spiro1985 PDFDokument4 SeitenSpiro1985 PDFNazihan Safitri AlkatiriNoch keine Bewertungen
- Exemplu 4Dokument4 SeitenExemplu 4Pavel SebastianNoch keine Bewertungen
- Headache After Removal of Vestibular Schwannoma Via The Retrosigmoid Approach: A Long-Term Follow-Up-StudyDokument9 SeitenHeadache After Removal of Vestibular Schwannoma Via The Retrosigmoid Approach: A Long-Term Follow-Up-StudySebastian GiovanniniNoch keine Bewertungen
- Occipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaDokument3 SeitenOccipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaMarcelo LambertiNoch keine Bewertungen
- Unsatisfactory Results After Tympanoplasty Surgery in Patients With Chronic Purulent Otitis MediaDokument4 SeitenUnsatisfactory Results After Tympanoplasty Surgery in Patients With Chronic Purulent Otitis MediaAcademic JournalNoch keine Bewertungen
- SS ArticleDokument8 SeitenSS ArticleWhite Feather Dental GurgaonNoch keine Bewertungen
- CT Scan For SinusitisDokument6 SeitenCT Scan For SinusitisYuke PutriNoch keine Bewertungen
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDokument7 SeitenOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040Noch keine Bewertungen
- Endoscopic Septoplasty: Indications, Technique, and ResultsDokument5 SeitenEndoscopic Septoplasty: Indications, Technique, and ResultsGabriel Vazquez RamosNoch keine Bewertungen
- Lawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseDokument4 SeitenLawrence Et Al 2021 Contralateral Transmaxillary Approach For Resection of Chondrosarcoma of The Petrous Apex A CaseSourabh PatroNoch keine Bewertungen
- Puccinelli 2019Dokument8 SeitenPuccinelli 2019RathavishwarajNoch keine Bewertungen
- 538-Article Text-7432-1-10-20200805Dokument8 Seiten538-Article Text-7432-1-10-20200805Ankita GuravNoch keine Bewertungen
- TurbinoplastyDokument7 SeitenTurbinoplastyNeena GuptaNoch keine Bewertungen
- Anatomical and Surgical Study of The Sphenopalatine Artery BranchesDokument5 SeitenAnatomical and Surgical Study of The Sphenopalatine Artery BranchesMarcelo DàvilaNoch keine Bewertungen
- Journal 2Dokument9 SeitenJournal 2Mathilda KinsalNoch keine Bewertungen
- Posterolateral Approach To The Craniocervical Junction.: Rully Hanafi Dahlan, SPBS, M.KesDokument2 SeitenPosterolateral Approach To The Craniocervical Junction.: Rully Hanafi Dahlan, SPBS, M.KesAdhitya Phemaw RahadiNoch keine Bewertungen
- JR 26 16Dokument5 SeitenJR 26 16ilomurtalaNoch keine Bewertungen
- Original Contributions: Joa O Gonc Alves Filho, MD, and Luiz Paulo Kowalski, MD, PHDDokument6 SeitenOriginal Contributions: Joa O Gonc Alves Filho, MD, and Luiz Paulo Kowalski, MD, PHDPrabjot SehmiNoch keine Bewertungen
- Bahan Ajar 9 SiringomieliaDokument5 SeitenBahan Ajar 9 SiringomieliaMuhammadKadafiNoch keine Bewertungen
- Combined Transnasal and Transoral Endoscopic Approaches To The Craniovertebral JunctionDokument6 SeitenCombined Transnasal and Transoral Endoscopic Approaches To The Craniovertebral JunctionRathavishwarajNoch keine Bewertungen
- A Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDokument6 SeitenA Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDay LightNoch keine Bewertungen
- Congress Auricular Reconstruction AbstractsDokument92 SeitenCongress Auricular Reconstruction AbstractsRocio RamirezNoch keine Bewertungen
- Epidural Anaesthesia For Laparoscopic CholecystectDokument1 SeiteEpidural Anaesthesia For Laparoscopic CholecystectAle GdzNoch keine Bewertungen
- Adenoma Hip1237Dokument6 SeitenAdenoma Hip1237isela castroNoch keine Bewertungen
- Chung2019 PDFDokument7 SeitenChung2019 PDFUmer HussainNoch keine Bewertungen
- The Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle DefectsDokument5 SeitenThe Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle Defectslia indria watiNoch keine Bewertungen
- EDJ - Volume 62 - Issue Issue 1 - January (Oral Surgery) - Pages 955-958Dokument4 SeitenEDJ - Volume 62 - Issue Issue 1 - January (Oral Surgery) - Pages 955-958Mohammed FaroukNoch keine Bewertungen
- Assessment of Racchimedular Injury by NursingVon EverandAssessment of Racchimedular Injury by NursingNoch keine Bewertungen
- Pediatric VaccineDokument354 SeitenPediatric VaccinePriya SahNoch keine Bewertungen
- Effectiveness of Tokyoguidelines 2018 in The Management of Acute Cholangitis and Acute CholecystitisDokument13 SeitenEffectiveness of Tokyoguidelines 2018 in The Management of Acute Cholangitis and Acute CholecystitisIJAR JOURNALNoch keine Bewertungen
- New Trends in Mechanical VentilationDokument4 SeitenNew Trends in Mechanical Ventilationashley_castro_4Noch keine Bewertungen
- Abdominal TraumaDokument41 SeitenAbdominal TraumaAhmad Shafwan NatsirNoch keine Bewertungen
- Aorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersDokument5 SeitenAorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersRudy DuterteNoch keine Bewertungen
- Visual PathwayDokument39 SeitenVisual Pathwayhuman anatomyNoch keine Bewertungen
- Activity 5: What Should One Do When Faced With A Medical Emergency Situation?Dokument3 SeitenActivity 5: What Should One Do When Faced With A Medical Emergency Situation?MarkBrendonJessVargasNoch keine Bewertungen
- Emergency MedicineDokument150 SeitenEmergency MedicineDev MartelNoch keine Bewertungen
- Seminar Report On Virtual SurgeryDokument17 SeitenSeminar Report On Virtual SurgeryAfrah RamsheedNoch keine Bewertungen
- Ureteroscopy G AdeyDokument66 SeitenUreteroscopy G AdeyCentanarianNoch keine Bewertungen
- Esophageal CancerDokument23 SeitenEsophageal Cancerabhandlung100% (3)
- Accidental Intra Arterial Injection Joel ArudchelvamDokument3 SeitenAccidental Intra Arterial Injection Joel ArudchelvamJoel Arudchelvam100% (1)
- Neuroanatomy FarreDokument2 SeitenNeuroanatomy FarreAbhay KumarNoch keine Bewertungen
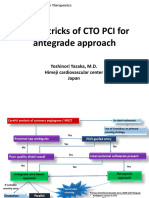
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDokument21 SeitenTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNoch keine Bewertungen
- Maternal Child Nursing ModuleDokument7 SeitenMaternal Child Nursing ModuleWizzardNoch keine Bewertungen
- Hudson Catalog PDFDokument91 SeitenHudson Catalog PDFNia PermanaNoch keine Bewertungen
- DR Rabiya Kaussar Tmo MCPS: Operative Vaginal DeliveryDokument45 SeitenDR Rabiya Kaussar Tmo MCPS: Operative Vaginal DeliveryHaseeb AwanNoch keine Bewertungen
- Entrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDokument2 SeitenEntrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDR RISKA WAHYUNoch keine Bewertungen
- ColostomyDokument4 SeitenColostomyleslie_macasaetNoch keine Bewertungen
- Development of MandibleDokument14 SeitenDevelopment of MandibleMahesh kumarNoch keine Bewertungen
- Rehabilitation of Cerebral Palsy & Motor DelayDokument49 SeitenRehabilitation of Cerebral Palsy & Motor DelayasloocltNoch keine Bewertungen
- Att 1446693658204 المذكرة-الذهبيةDokument80 SeitenAtt 1446693658204 المذكرة-الذهبيةShady KhamisNoch keine Bewertungen
- Dr. Risma Dikirim Pukul 0 16sympo OptimizingDokument30 SeitenDr. Risma Dikirim Pukul 0 16sympo OptimizingAlthof SonaNoch keine Bewertungen
- Anesthesia For ERCP PDFDokument3 SeitenAnesthesia For ERCP PDFHarish BhatNoch keine Bewertungen
- Resume - Parand GheshlaghiDokument3 SeitenResume - Parand Gheshlaghimohammadrezahajian12191Noch keine Bewertungen
- Principles of SterilityDokument25 SeitenPrinciples of SterilityjuliusromatolentinoNoch keine Bewertungen
- Ob Journal 2Dokument3 SeitenOb Journal 2api-662323379Noch keine Bewertungen
- PTMC Percutaneous Balloon Mitral Valvuloplasty (PBMV) .NicvdDokument42 SeitenPTMC Percutaneous Balloon Mitral Valvuloplasty (PBMV) .NicvdNavojit Chowdhury100% (1)
- Nitrous Oxide Inhalation Is A Safe and Effective Way To Facilitate Procedures in Paediatric Outpatient DepartmentsDokument4 SeitenNitrous Oxide Inhalation Is A Safe and Effective Way To Facilitate Procedures in Paediatric Outpatient DepartmentsfebyNoch keine Bewertungen