Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Manual Mmpi 2 PDFDokument3 SeitenManual Mmpi 2 PDFSana Sajid17% (12)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Basavaraj-Colour Therapy PDFDokument144 SeitenBasavaraj-Colour Therapy PDFTanuku Net86% (14)
- 4 Hypovolemic ShockDokument21 Seiten4 Hypovolemic Shocksayednour100% (4)
- What Robotic Re-Embodiment Reveals About Virtual Re-EmbodimentDokument17 SeitenWhat Robotic Re-Embodiment Reveals About Virtual Re-Embodimentherac12Noch keine Bewertungen
- Fluid Electrolytes and Acid Base BalanceDokument108 SeitenFluid Electrolytes and Acid Base BalancesayednourNoch keine Bewertungen
- Basics of Laser Orthopedic ViewDokument24 SeitenBasics of Laser Orthopedic ViewsayednourNoch keine Bewertungen
- Assessment of Suitability For Lung Resection: Gerard Gould FRCA Adrian Pearce FRCADokument4 SeitenAssessment of Suitability For Lung Resection: Gerard Gould FRCA Adrian Pearce FRCAsayednourNoch keine Bewertungen
- Anesthesia in The FutureDokument11 SeitenAnesthesia in The FuturesayednourNoch keine Bewertungen
- An Overview of Therapeutic Plasma ExchangeDokument65 SeitenAn Overview of Therapeutic Plasma ExchangesayednourNoch keine Bewertungen
- General Anesthesia For Cesarean SectionDokument33 SeitenGeneral Anesthesia For Cesarean Sectionsayednour100% (2)
- AnestheticsDokument34 SeitenAnestheticssayednourNoch keine Bewertungen
- 166 Serotonin SyndromeDokument5 Seiten166 Serotonin SyndromesayednourNoch keine Bewertungen
- 1 Plasmapheresis - 1Dokument61 Seiten1 Plasmapheresis - 1sayednour100% (1)
- Plasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?Dokument4 SeitenPlasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?sayednourNoch keine Bewertungen
- Adrenal CrisisDokument27 SeitenAdrenal CrisissayednourNoch keine Bewertungen
- Nitric Oxide An Overview: Salwa Hassan Teama M.D. NCI. Cairo UniversityDokument31 SeitenNitric Oxide An Overview: Salwa Hassan Teama M.D. NCI. Cairo Universitysayednour100% (1)
- Review Mechanisms of Glucocorticoid-Induced Myopathy: O Schakman, H Gilson and J P ThissenDokument10 SeitenReview Mechanisms of Glucocorticoid-Induced Myopathy: O Schakman, H Gilson and J P ThissensayednourNoch keine Bewertungen
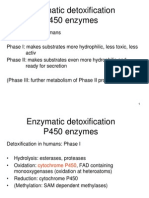
- Enzymatic Detoxification P450 EnzymesDokument22 SeitenEnzymatic Detoxification P450 EnzymessayednourNoch keine Bewertungen
- Cohort StudyDokument31 SeitenCohort Studysayednour50% (2)
- Tony Chang, MD Tuesday Conference September 6, 2005Dokument75 SeitenTony Chang, MD Tuesday Conference September 6, 2005sayednourNoch keine Bewertungen
- Developmental Genetics and Pharmacogeneticsdoc4301Dokument8 SeitenDevelopmental Genetics and Pharmacogeneticsdoc4301sayednourNoch keine Bewertungen
- 8 Plasma Derivatives ProductsDokument12 Seiten8 Plasma Derivatives ProductssayednourNoch keine Bewertungen
- 185 Anaesthesia in Pregnancy For Non Obstetric SurgeryDokument9 Seiten185 Anaesthesia in Pregnancy For Non Obstetric SurgeryaangrohmananiaNoch keine Bewertungen
- Hennebert's SignDokument3 SeitenHennebert's SignatmhyaNoch keine Bewertungen
- Selina Solutions For Class 10 Biology Chapter 11 Sense OrgansDokument19 SeitenSelina Solutions For Class 10 Biology Chapter 11 Sense OrgansParardha DharNoch keine Bewertungen
- Intelligence Testing On WISCDokument60 SeitenIntelligence Testing On WISCSangeeta ParabNoch keine Bewertungen
- Coordination & Response 5 QP PDFDokument6 SeitenCoordination & Response 5 QP PDFJeffrey PiggottNoch keine Bewertungen
- Neuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline MalformationDokument13 SeitenNeuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline Malformationfamiliesforhope100% (1)
- Bipolar PowerpointDokument10 SeitenBipolar PowerpointRAYMIND MIRANDANoch keine Bewertungen
- CHAPTER 1the Mind-Brain RelationshipDokument23 SeitenCHAPTER 1the Mind-Brain RelationshipRain Simonette GuanNoch keine Bewertungen
- CgassDokument3 SeitenCgassComan CristinaNoch keine Bewertungen
- Neurofilament Light Chain Gaetani2019Dokument12 SeitenNeurofilament Light Chain Gaetani2019eastareaNoch keine Bewertungen
- Nursing Care PlanDokument3 SeitenNursing Care Plansarah hanaNoch keine Bewertungen
- C9apstudy GuideDokument37 SeitenC9apstudy GuidejqtdNoch keine Bewertungen
- 단어시험 (Day 4~6)Dokument15 Seiten단어시험 (Day 4~6)qkrwldnjs0314Noch keine Bewertungen
- Thigmonasty 1Dokument3 SeitenThigmonasty 1BeaNoch keine Bewertungen
- Neuropsychology 2 BetDokument11 SeitenNeuropsychology 2 BetMike TemboNoch keine Bewertungen
- SSR Disability Services CentreDokument3 SeitenSSR Disability Services CentreIrshaad Ally Ashrafi GolapkhanNoch keine Bewertungen
- CIDP UpToDateDokument7 SeitenCIDP UpToDatesvd2009Noch keine Bewertungen
- Full Test Bank For Essentials of Psychology 7Th Edition Douglas A Bernstein PDF Docx Full Chapter ChapterDokument36 SeitenFull Test Bank For Essentials of Psychology 7Th Edition Douglas A Bernstein PDF Docx Full Chapter Chapterbethmcneilysgbzqkpnw100% (11)
- Philip Kosovrasti - Resource GuideDokument9 SeitenPhilip Kosovrasti - Resource Guideapi-340370776Noch keine Bewertungen
- Midterms Reviewer Ana 2Dokument8 SeitenMidterms Reviewer Ana 2Ais WallensteinNoch keine Bewertungen
- Blue BrainDokument19 SeitenBlue BrainDanielle HoltNoch keine Bewertungen
- Anatomy of The Eye WorksheetDokument1 SeiteAnatomy of The Eye WorksheetIrfan ArifNoch keine Bewertungen
- Morning Report: Departement of Neurology m28 Muhammadiyah Lamongan HospitalDokument19 SeitenMorning Report: Departement of Neurology m28 Muhammadiyah Lamongan HospitalratnaNoch keine Bewertungen
- Dopamine D3 Receptor - A Neglected Participant in Parkinson Disease Pathogenesis and Treatment?Dokument45 SeitenDopamine D3 Receptor - A Neglected Participant in Parkinson Disease Pathogenesis and Treatment?Daniel TorresNoch keine Bewertungen
- PTSD and Cognitive Processing Therapy Presented by Patricia A. Resick, PHD, AbppDokument28 SeitenPTSD and Cognitive Processing Therapy Presented by Patricia A. Resick, PHD, AbppDardo Arreche100% (2)
- A Metacognitive Therapy For Anxiety Disorders - Buddhist Psychology Applied (2002 Cognitive and B PDFDokument7 SeitenA Metacognitive Therapy For Anxiety Disorders - Buddhist Psychology Applied (2002 Cognitive and B PDFclaudiaghergariNoch keine Bewertungen
- Pathological Demand Avoidance and The DSM-5: A Rebuttal To Judy EatonDokument4 SeitenPathological Demand Avoidance and The DSM-5: A Rebuttal To Judy EatonyeyesNoch keine Bewertungen
- Vielight Inventors Notes For Neuro Alpha and Neuro Gamma 2017Dokument17 SeitenVielight Inventors Notes For Neuro Alpha and Neuro Gamma 2017arexixNoch keine Bewertungen