Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Vaccine IngredientsDokument7 SeitenVaccine IngredientsShoshannah100% (22)
- Epidemiology Triangle of MalariaDokument3 SeitenEpidemiology Triangle of MalariaArslan Bashir100% (8)
- 2021.07.21 LWV Corpus Christi Lead Contamination in Drinking Water Study & Position Statement - NCDokument13 Seiten2021.07.21 LWV Corpus Christi Lead Contamination in Drinking Water Study & Position Statement - NCcallertimesNoch keine Bewertungen
- PIS DR SamiDokument1 SeitePIS DR SamiSami HassanNoch keine Bewertungen
- Essential Newborn CareDokument14 SeitenEssential Newborn CareJam Corros100% (1)
- Influenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionDokument3 SeitenInfluenza: Flu "Influenza" Definition, Symptoms, Causes, Treatment, PreventionYusuf Rony LosongNoch keine Bewertungen
- Guideline URTI in South Africa 2008Dokument9 SeitenGuideline URTI in South Africa 2008Febbe Nadia Okky LucianaNoch keine Bewertungen
- Coast Guard Public School, Daman: (Type Here)Dokument13 SeitenCoast Guard Public School, Daman: (Type Here)Rajeev SinghNoch keine Bewertungen
- Endometrial BiopsyDokument9 SeitenEndometrial BiopsyAnna BartolomeNoch keine Bewertungen
- Neonatal InfectionDokument18 SeitenNeonatal InfectionchinchuNoch keine Bewertungen
- Indonesia Country ProfileDokument4 SeitenIndonesia Country ProfilegitasariaryaniNoch keine Bewertungen
- Abnormal Uterine BleedingDokument22 SeitenAbnormal Uterine BleedingAde JuandaNoch keine Bewertungen
- Vaccination Myths - A. G. PhillipsDokument11 SeitenVaccination Myths - A. G. PhillipsBrendan D. MurphyNoch keine Bewertungen
- Hawiyah Gas Plant Expansion: Basic Safety Instructions For All Employees Working atDokument10 SeitenHawiyah Gas Plant Expansion: Basic Safety Instructions For All Employees Working atmalik jahanNoch keine Bewertungen
- Condom Ad Ban India OrderDokument2 SeitenCondom Ad Ban India OrderPrasun TiwariNoch keine Bewertungen
- Ijogr 6 4 444 447Dokument4 SeitenIjogr 6 4 444 447RachnaNoch keine Bewertungen
- Key Components of Industrial HygieneDokument2 SeitenKey Components of Industrial HygieneCharlotte LibreroNoch keine Bewertungen
- Philippine National Environmental Health Action Plan (2017-2022)Dokument106 SeitenPhilippine National Environmental Health Action Plan (2017-2022)Boni MagtibayNoch keine Bewertungen
- Epidemiology NewDokument26 SeitenEpidemiology NewBabita DhruwNoch keine Bewertungen
- OCHA PH - Measles OutbreakDokument1 SeiteOCHA PH - Measles OutbreakPhilippe Ceasar C. BascoNoch keine Bewertungen
- Medstar ObGyn 2nd EditionDokument570 SeitenMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- What Are The Advantages and Disadvantages of Breastfeeding?Dokument3 SeitenWhat Are The Advantages and Disadvantages of Breastfeeding?K EV INNoch keine Bewertungen
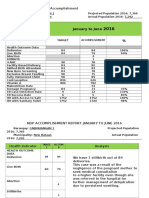
- Bhs Andap NDP Accomplishment ReportDokument4 SeitenBhs Andap NDP Accomplishment ReportRonald A. SagangNoch keine Bewertungen
- Pengaruh Senam Kaki Terhadap Kadar Glukosa Darah Dan Nilai ABI Penderita DMDokument6 SeitenPengaruh Senam Kaki Terhadap Kadar Glukosa Darah Dan Nilai ABI Penderita DMSetyardiNoch keine Bewertungen
- Sample of A Project Proposal Water System ProjectDokument8 SeitenSample of A Project Proposal Water System ProjectJomari Sinaban100% (3)
- UOA - Cold Water Pipe SizingDokument4 SeitenUOA - Cold Water Pipe SizingDuoc Su HoangNoch keine Bewertungen
- Yahaya Musa Balarabe's Project CHAPTER ONE To ThreeDokument25 SeitenYahaya Musa Balarabe's Project CHAPTER ONE To ThreeJonah MerabNoch keine Bewertungen
- Dog Bite 3Dokument2 SeitenDog Bite 3ElvisNoch keine Bewertungen
- Epi 3rd Exam ReviewerDokument93 SeitenEpi 3rd Exam ReviewerJillian AsdalaNoch keine Bewertungen
- INFOSAN User Guide FinalDokument17 SeitenINFOSAN User Guide FinalJorge Gregorio SeguraNoch keine Bewertungen