Das könnte Ihnen auch gefallen
- Normal Variant in Abdominal UltrasounDokument20 SeitenNormal Variant in Abdominal Ultrasounshanks spearsonNoch keine Bewertungen
- Scanning Technique of KidneysDokument103 SeitenScanning Technique of KidneysPhuntsho OngmoNoch keine Bewertungen
- Basics of Abdominal UltrasonographyDokument141 SeitenBasics of Abdominal UltrasonographyalmoslihNoch keine Bewertungen
- Scrotum Protocol 14Dokument2 SeitenScrotum Protocol 14api-349402240Noch keine Bewertungen
- Fetal Echocardiogram ProtocolDokument4 SeitenFetal Echocardiogram Protocolapi-349402240Noch keine Bewertungen
- Ob Biophysical Profile Protocol r14 PDFDokument3 SeitenOb Biophysical Profile Protocol r14 PDFapi-390240132Noch keine Bewertungen
- Abdomen Protocol 14 PDFDokument6 SeitenAbdomen Protocol 14 PDFapi-390240132Noch keine Bewertungen
- Lower Extremity Arterial Protocol 14 PDFDokument2 SeitenLower Extremity Arterial Protocol 14 PDFapi-390240132Noch keine Bewertungen
- LiverultrasoundDokument62 SeitenLiverultrasoundiuliia94Noch keine Bewertungen
- Kuliah Blok GI Tract - USG Abd - September 2010Dokument65 SeitenKuliah Blok GI Tract - USG Abd - September 2010Natallia BatuwaelNoch keine Bewertungen
- Upper Extremity Arterial Protocol 14 PDFDokument2 SeitenUpper Extremity Arterial Protocol 14 PDFapi-390240132Noch keine Bewertungen
- 超声进展2020 10 8最终版Dokument160 Seiten超声进展2020 10 8最终版Wai Kwong ChiuNoch keine Bewertungen
- Renal Ultrasound ProtocolDokument4 SeitenRenal Ultrasound Protocolfouad tabetNoch keine Bewertungen
- 9 Muscle Teaching Slides PDFDokument91 Seiten9 Muscle Teaching Slides PDFhosam jaradatNoch keine Bewertungen
- Pediatric Echocardiography: Understanding Congenital Heart DefectsDokument159 SeitenPediatric Echocardiography: Understanding Congenital Heart DefectsSergiu NiculitaNoch keine Bewertungen
- Us Vasos RetroperitonealesDokument101 SeitenUs Vasos RetroperitonealesLourdes MarcosNoch keine Bewertungen
- Policies and Statements: Peripheral Arterial UltrasoundDokument5 SeitenPolicies and Statements: Peripheral Arterial UltrasoundJing CruzNoch keine Bewertungen
- D5 PolicyDokument5 SeitenD5 PolicyDenis PogoreviciNoch keine Bewertungen
- Penis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsDokument35 SeitenPenis Sonography. A Pictorial Review: Poster No.: Congress: Type: AuthorsOky Sutarto PutraNoch keine Bewertungen
- Us Abdominal AortaDokument16 SeitenUs Abdominal AortaRomaNoch keine Bewertungen
- Penile US and Doppler USDokument2 SeitenPenile US and Doppler UShardrocker_2007Noch keine Bewertungen
- Upper Extremity Venous Protocol 14Dokument2 SeitenUpper Extremity Venous Protocol 14api-349402240Noch keine Bewertungen
- Renal Ultrasound: Diana Pancu, MDDokument76 SeitenRenal Ultrasound: Diana Pancu, MDReza Angga PratamaNoch keine Bewertungen
- Head and Neck Gastrointestinal Lung Pelvic Renal and BladderDokument10 SeitenHead and Neck Gastrointestinal Lung Pelvic Renal and BladderAmir AliNoch keine Bewertungen
- Gynecoloical Ultrasound Doppler AssessmentDokument17 SeitenGynecoloical Ultrasound Doppler AssessmentKinzaNoch keine Bewertungen
- Diagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MDokument70 SeitenDiagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MDea Amelia YolandaNoch keine Bewertungen
- High-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsDokument41 SeitenHigh-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsAlvin JulianNoch keine Bewertungen
- Small Parts USDokument58 SeitenSmall Parts USWaqas AliNoch keine Bewertungen
- Lower Extremity Venous Protocol 14Dokument3 SeitenLower Extremity Venous Protocol 14api-276847924Noch keine Bewertungen
- The Kidney: Dr. I Made Naris Pujawan, M.Biomed, SP - PADokument18 SeitenThe Kidney: Dr. I Made Naris Pujawan, M.Biomed, SP - PAIda AyuNoch keine Bewertungen
- Ultrasonography of The Hepatobiliary TractDokument9 SeitenUltrasonography of The Hepatobiliary TractPaola Méndez NeciosupNoch keine Bewertungen
- Normal Reference Values: DR Ayush GoelDokument2 SeitenNormal Reference Values: DR Ayush GoelNic WGTNoch keine Bewertungen
- ECR2014 - Ultrasound Evaluation of Scrotal PathologyDokument76 SeitenECR2014 - Ultrasound Evaluation of Scrotal PathologyMicNoch keine Bewertungen
- Doppler US and GrowthDokument43 SeitenDoppler US and GrowthAulia rahmawatiNoch keine Bewertungen
- Basic Ultasonograph yDokument56 SeitenBasic Ultasonograph yshashwathhNoch keine Bewertungen
- 93306Dokument64 Seiten93306jamesgailNoch keine Bewertungen
- Biophysical Profile& Color Doppler Ultrasound in The High Risk PregnancyDokument56 SeitenBiophysical Profile& Color Doppler Ultrasound in The High Risk Pregnancykhadzx100% (4)
- To Review The Imaging Anatomy of Peritoneal Spaces: Poster No.: Congress: Type: Authors: Keywords: DoiDokument20 SeitenTo Review The Imaging Anatomy of Peritoneal Spaces: Poster No.: Congress: Type: Authors: Keywords: DoiradiologirsckNoch keine Bewertungen
- QA and ProtocolsDokument112 SeitenQA and Protocolsayesha rafiq sheikhNoch keine Bewertungen
- Appendix Protocol 14 1Dokument2 SeitenAppendix Protocol 14 1api-349402240Noch keine Bewertungen
- #Normal #Tubes On #UltrasoundDokument1 Seite#Normal #Tubes On #UltrasoundDr Pankaj TalwarNoch keine Bewertungen
- Normal Ovaries On UltrasoundDokument1 SeiteNormal Ovaries On UltrasoundDr Pankaj TalwarNoch keine Bewertungen
- Articulo Tesis 6Dokument130 SeitenArticulo Tesis 6Lourdes MarcosNoch keine Bewertungen
- Doppler Ultrasound of The KidneysDokument23 SeitenDoppler Ultrasound of The KidneysivoklarinNoch keine Bewertungen
- Handbook of Transrectal Ultrasound and Biopsy of The ProstateDokument126 SeitenHandbook of Transrectal Ultrasound and Biopsy of The ProstateIván RomeroNoch keine Bewertungen
- Breast Procedures Ultrasound Only EditedDokument107 SeitenBreast Procedures Ultrasound Only EditedDanaNoch keine Bewertungen
- Lower Extremity Arterial Protocol 14 1Dokument2 SeitenLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Extrahepatic Biliary ObstructionDokument44 SeitenExtrahepatic Biliary ObstructionOssama Abd Al-amierNoch keine Bewertungen
- Baltarowich ABD pt1 Hepatobiliary US PDFDokument22 SeitenBaltarowich ABD pt1 Hepatobiliary US PDFEka KusumaningatiNoch keine Bewertungen
- Cranial Ultrasound: A Guide to Sonographic Technique and PathologiesDokument43 SeitenCranial Ultrasound: A Guide to Sonographic Technique and PathologiesJazib ShahidNoch keine Bewertungen
- Renal Doppler Protocol 14 1Dokument4 SeitenRenal Doppler Protocol 14 1api-349402240100% (1)
- Mesenteric Doppler Protocol 14Dokument2 SeitenMesenteric Doppler Protocol 14api-349402240Noch keine Bewertungen
- 3881825Dokument30 Seiten3881825saryindrianyNoch keine Bewertungen
- Ultrasound of Srotal Emergency in PediatricDokument53 SeitenUltrasound of Srotal Emergency in PediatricIsti Iryan PriantiNoch keine Bewertungen
- Liver Protocol 14 1Dokument5 SeitenLiver Protocol 14 1api-349402240Noch keine Bewertungen
- Normal Fetal Anatomy2Dokument26 SeitenNormal Fetal Anatomy2swati100% (1)
- Pediatric Spine 14Dokument2 SeitenPediatric Spine 14api-349402240Noch keine Bewertungen
- Women's Imaging: MRI with Multimodality CorrelationVon EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownBewertung: 5 von 5 Sternen5/5 (1)
- Echocardiography in Pediatric and Congenital Heart Disease: From Fetus to AdultVon EverandEchocardiography in Pediatric and Congenital Heart Disease: From Fetus to AdultNoch keine Bewertungen
- Ruby and Pink Sapphire - IntroDokument3 SeitenRuby and Pink Sapphire - Introrazanym100% (1)
- Yara Crop Nutrition For HorticultureDokument8 SeitenYara Crop Nutrition For HorticultureadjieNoch keine Bewertungen
- Lesson Plan 2aDokument5 SeitenLesson Plan 2aapi-332424736Noch keine Bewertungen
- Network FYPDokument3 SeitenNetwork FYPla tahzanNoch keine Bewertungen
- Diversification in Flavoured Milk: A ReviewDokument6 SeitenDiversification in Flavoured Milk: A ReviewInternational Journal of Clinical and Biomedical Research (IJCBR)Noch keine Bewertungen
- Output Configurations and Connections: NPN Open CollectorDokument2 SeitenOutput Configurations and Connections: NPN Open Collectordorin serbanNoch keine Bewertungen
- CSS9 TQ PT 3rd4thDokument8 SeitenCSS9 TQ PT 3rd4thJevan Hope BaltazarNoch keine Bewertungen
- SynopsisDokument13 SeitenSynopsisharivijay ranmaleNoch keine Bewertungen
- University of Toronto Astronomy 101 Midterm Test QuestionsDokument6 SeitenUniversity of Toronto Astronomy 101 Midterm Test QuestionsTrash RowzanNoch keine Bewertungen
- GPS Navigator: ModelDokument99 SeitenGPS Navigator: ModelMain UddinNoch keine Bewertungen
- Transmission Lines Explained for Efficiency and Loss ReductionDokument25 SeitenTransmission Lines Explained for Efficiency and Loss Reductionjagdish choudharyNoch keine Bewertungen
- Ashrae 62.1-2019Dokument92 SeitenAshrae 62.1-2019Alejandro Castillo100% (16)
- Therapeutic Drug Monitoring GuideDokument12 SeitenTherapeutic Drug Monitoring GuidePromise NcubeNoch keine Bewertungen
- 123 Rule For TRS MMD DG ShippingDokument2 Seiten123 Rule For TRS MMD DG ShippingGurjit SinghNoch keine Bewertungen
- Caterpillar FAPT Presentation PDFDokument18 SeitenCaterpillar FAPT Presentation PDFJuniOrs RiVeraNoch keine Bewertungen
- Raise The Limits: Eppendorf Research PlusDokument12 SeitenRaise The Limits: Eppendorf Research PlusZahia Slama Ep AchourNoch keine Bewertungen
- Section 09 - Traction Electrification SystemDokument47 SeitenSection 09 - Traction Electrification SystemAbu Monsur Ali100% (1)
- 6013 GCS-CONTROLS enDokument5 Seiten6013 GCS-CONTROLS enMuhammad SyaqirinNoch keine Bewertungen
- Oral Hygiene: Presented By: Anis Anis Andreas KyriakidisDokument60 SeitenOral Hygiene: Presented By: Anis Anis Andreas Kyriakidislenami_91Noch keine Bewertungen
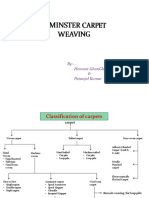
- Axminster CarpetDokument19 SeitenAxminster Carpetrohit sinhaNoch keine Bewertungen
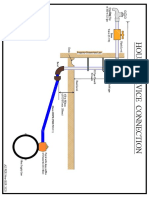
- House Service Connection NEW BSR 2020-1Dokument1 SeiteHouse Service Connection NEW BSR 2020-1Deshraj BairwaNoch keine Bewertungen
- Mahamrityunjaya MantraDokument8 SeitenMahamrityunjaya MantraBalakrishnan KannanNoch keine Bewertungen
- End UserDokument205 SeitenEnd Userghica05Noch keine Bewertungen
- Ajhgaa English O6Dokument28 SeitenAjhgaa English O6dhirumeshkumarNoch keine Bewertungen
- Design of Goods & Services: Tanweer Ascem KharralDokument10 SeitenDesign of Goods & Services: Tanweer Ascem KharralHadeed GulNoch keine Bewertungen
- E5971 m4n68t-m Series ManualDokument0 SeitenE5971 m4n68t-m Series ManualcamiloelosadaNoch keine Bewertungen
- CP I-O Modules PDFDokument91 SeitenCP I-O Modules PDFVlad ChioreanNoch keine Bewertungen
- Connorized Classical CatalogDokument37 SeitenConnorized Classical CatalogPablo Olea RodríguezNoch keine Bewertungen
- Din en 50155 (Vde 0115-200) - 2008-03Dokument42 SeitenDin en 50155 (Vde 0115-200) - 2008-03Collins Akhimien100% (1)
- Aspirasi MekoniumDokument17 SeitenAspirasi MekoniumimanNoch keine Bewertungen