Das könnte Ihnen auch gefallen
- Pulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseVon EverandPulmonary Assessment and Management of Patients with Pediatric Neuromuscular DiseaseOscar Henry MayerNoch keine Bewertungen
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)Von EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)Noch keine Bewertungen
- Materi Kuliah ArdsDokument38 SeitenMateri Kuliah ArdsHadiah ArdianiNoch keine Bewertungen
- VM PediatrikDokument13 SeitenVM PediatrikWayan SupiartaNoch keine Bewertungen
- The Role of High-Frequency Ventilation in Neonates: Evidence-Based RecommendationsDokument16 SeitenThe Role of High-Frequency Ventilation in Neonates: Evidence-Based RecommendationsSiska LesnussaNoch keine Bewertungen
- Permissive Hypercapnia in Extremely Low Birthweight Infants (PHELBI) : A Randomised Controlled Multicentre Trial LancetDokument13 SeitenPermissive Hypercapnia in Extremely Low Birthweight Infants (PHELBI) : A Randomised Controlled Multicentre Trial LancetJane LlasiNoch keine Bewertungen
- BPD Pathogen Es IsDokument10 SeitenBPD Pathogen Es IsTriponiaNoch keine Bewertungen
- Ards PicucourseDokument58 SeitenArds PicucoursesurasuarezlopezNoch keine Bewertungen
- Articulo ViernesDokument6 SeitenArticulo Viernesvelf5Noch keine Bewertungen
- Bronquilitis Pdiatrics 2010Dokument10 SeitenBronquilitis Pdiatrics 2010thorin8Noch keine Bewertungen
- Staff Pengajar Fik Ui: Made Kariasa, Skp.,Mm.,Mkep.,Sp - MB.,PG - CertDokument37 SeitenStaff Pengajar Fik Ui: Made Kariasa, Skp.,Mm.,Mkep.,Sp - MB.,PG - CertRini Fauzia ANoch keine Bewertungen
- A Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisDokument11 SeitenA Randomized Trial of High-Flow Oxygen Therapy in Infants With BronchiolitisErwin YanthoNoch keine Bewertungen
- PathoPhysiology of Ards 2017Dokument22 SeitenPathoPhysiology of Ards 2017Andi sutandiNoch keine Bewertungen
- Rclutamiento VAFO Pre Surfactante PTDokument7 SeitenRclutamiento VAFO Pre Surfactante PTGustavo Carhuamaca RoblesNoch keine Bewertungen
- Pediatric Respiratory OMT ModuleDokument51 SeitenPediatric Respiratory OMT ModuleTameemNoch keine Bewertungen
- Ebook Kendigs Disorders of The Respiratory Tract in Children PDF Full Chapter PDFDokument67 SeitenEbook Kendigs Disorders of The Respiratory Tract in Children PDF Full Chapter PDFbilly.greco742100% (29)
- Crit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopDokument11 SeitenCrit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopTharshini_Indr_6713Noch keine Bewertungen
- AsthmaDokument17 SeitenAsthmaphobicmdNoch keine Bewertungen
- Management and Treatment Guidelines For Sepsis in Pediatric PatientsDokument9 SeitenManagement and Treatment Guidelines For Sepsis in Pediatric PatientsIhsan PutraNoch keine Bewertungen
- 9mechanical Ventilation in Sepsis-Induced Acute LungDokument6 Seiten9mechanical Ventilation in Sepsis-Induced Acute LungTeodora ZamfirescuNoch keine Bewertungen
- 1 - Bronchopulmonary DysplasiaDokument16 Seiten1 - Bronchopulmonary DysplasiaBirtukanNoch keine Bewertungen
- Kendigs Disorders of The Respiratory Tract in Children 9Th Edition Robert W Wilmott Full ChapterDokument50 SeitenKendigs Disorders of The Respiratory Tract in Children 9Th Edition Robert W Wilmott Full Chapterernest.guzman635100% (5)
- 6Dokument16 Seiten6delphineNoch keine Bewertungen
- ARDS LectureDokument58 SeitenARDS LecturedrjaikrishNoch keine Bewertungen
- RCT of Aprv Vs LPV in Ards PtsDokument11 SeitenRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariNoch keine Bewertungen
- Sol Hipert en SibilanciasDokument9 SeitenSol Hipert en Sibilanciasedith sandovalNoch keine Bewertungen
- Chest Physiotherapy in Mechanically Ventilated Children A ReviewDokument10 SeitenChest Physiotherapy in Mechanically Ventilated Children A Reviewmrizki_1Noch keine Bewertungen
- Respiratory Distress SyndromeDokument7 SeitenRespiratory Distress SyndromeBilal RowaihiNoch keine Bewertungen
- Myeloperoxidase and Protein Oxidation in The Airways of Young Children With Cystic FibrosisDokument7 SeitenMyeloperoxidase and Protein Oxidation in The Airways of Young Children With Cystic FibrosisMichael StudiofourteenohnineNoch keine Bewertungen
- Abnormal InfantDokument8 SeitenAbnormal InfantSal Ie EmNoch keine Bewertungen
- CDH and Pulmonary HypertensionDokument6 SeitenCDH and Pulmonary HypertensionStollery SandboxNoch keine Bewertungen
- Lung Injury in NeonatesDokument9 SeitenLung Injury in NeonateszunarodriguezleoNoch keine Bewertungen
- ArdsDokument81 SeitenArdsAmit KlNoch keine Bewertungen
- Pulmonary Interstitial Emphysema Complicating Pneumonia in An Unventilated Term InfantDokument3 SeitenPulmonary Interstitial Emphysema Complicating Pneumonia in An Unventilated Term Infantindra_poetoetNoch keine Bewertungen
- 693 FullDokument12 Seiten693 FullGilmer alvarez floresNoch keine Bewertungen
- Joseph J. Zorc Caroline Breese Hall: Bronchiolitis: Recent Evidence On Diagnosis and Management, MD, Msce, ,, MDDokument10 SeitenJoseph J. Zorc Caroline Breese Hall: Bronchiolitis: Recent Evidence On Diagnosis and Management, MD, Msce, ,, MDArie PrasetyowatiNoch keine Bewertungen
- The Acute Respiratory Distress Syndrome in 2013: Review Open AccessDokument6 SeitenThe Acute Respiratory Distress Syndrome in 2013: Review Open Accessindriyanti natasya ayu utami kottenNoch keine Bewertungen
- Treatment PDADokument8 SeitenTreatment PDAijaldo ajahNoch keine Bewertungen
- Articulos BronquiolitisDokument18 SeitenArticulos BronquiolitisLaura López Del Castillo LalydelcaNoch keine Bewertungen
- Ventilatory Strategies in Obstructive Lung. Parrilla2014Dokument10 SeitenVentilatory Strategies in Obstructive Lung. Parrilla2014EzeBorjesNoch keine Bewertungen
- The Acute Respiratory Distress Syndrome: Review SeriesDokument10 SeitenThe Acute Respiratory Distress Syndrome: Review Seriesadek07Noch keine Bewertungen
- Dasenbrook higherPEEP 11 PrintedDokument8 SeitenDasenbrook higherPEEP 11 PrintedОлег СатишурNoch keine Bewertungen
- Prophylaxis and Treatment For AspirationDokument19 SeitenProphylaxis and Treatment For Aspirationbalab2311Noch keine Bewertungen
- Intensive Care Nursery House Staff ManualDokument9 SeitenIntensive Care Nursery House Staff ManualVenus MargaretteNoch keine Bewertungen
- Conti 2016Dokument7 SeitenConti 2016Dwi Putri SekariniNoch keine Bewertungen
- Ecmo 2017Dokument19 SeitenEcmo 2017Josefina Daza SantamaríaNoch keine Bewertungen
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDokument16 SeitenAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelNoch keine Bewertungen
- Accepted Manuscript: Paediatric Respiratory ReviewsDokument16 SeitenAccepted Manuscript: Paediatric Respiratory ReviewsAlvaro Guillen CerpaNoch keine Bewertungen
- JACOB 1998 - Long-Term Pulmonary Sequelae of Severe Bronchopulmonary DysplasiaDokument8 SeitenJACOB 1998 - Long-Term Pulmonary Sequelae of Severe Bronchopulmonary DysplasiaRafael JustinoNoch keine Bewertungen
- RSV - PPCDokument36 SeitenRSV - PPCchinokenjiNoch keine Bewertungen
- Recommendation 1ADokument26 SeitenRecommendation 1Asyahrizon thomasNoch keine Bewertungen
- Hassinger 2014Dokument8 SeitenHassinger 2014Angelica Lucero OrtizNoch keine Bewertungen
- Fluminant Pertussis PDFDokument11 SeitenFluminant Pertussis PDFDooriitha Pérez Peralta100% (1)
- Effectiveness of Airway ClearanceDokument7 SeitenEffectiveness of Airway ClearanceNelly Lutfieta SariNoch keine Bewertungen
- Klebsiella PDFDokument4 SeitenKlebsiella PDFOscarEduardoNoch keine Bewertungen
- Acute Respiratory Distress Syndrome (ARDS)Dokument85 SeitenAcute Respiratory Distress Syndrome (ARDS)Jose Adan Vazquez MoralesNoch keine Bewertungen
- Resp Emer in ChildrenDokument35 SeitenResp Emer in ChildrenvgmanjunathNoch keine Bewertungen
- Bronquiolitis - Pediatrics, Feb 2010Dokument10 SeitenBronquiolitis - Pediatrics, Feb 2010Luis RodasNoch keine Bewertungen
- Bronchilitis PediatricsDokument10 SeitenBronchilitis PediatricsJoseph Arzapalo BenavidesNoch keine Bewertungen
- How Was The Distribution of Clothes and Medicines That Poured in For The Tsunami Victims Handled? (4marks)Dokument12 SeitenHow Was The Distribution of Clothes and Medicines That Poured in For The Tsunami Victims Handled? (4marks)Kota VinayNoch keine Bewertungen
- Premature Ventricular Contractions: Ralph Augostini, MD FACC FHRSDokument33 SeitenPremature Ventricular Contractions: Ralph Augostini, MD FACC FHRSLivianty HukubunNoch keine Bewertungen
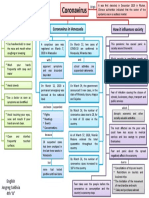
- Mapa Mental Coronavirus en InglesDokument1 SeiteMapa Mental Coronavirus en InglestavimayrNoch keine Bewertungen
- Infection Control Questions For StaffDokument3 SeitenInfection Control Questions For StaffManisha maharaNoch keine Bewertungen
- A Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentDokument4 SeitenA Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentEditor_IAIMNoch keine Bewertungen
- Uropathy The Most Powerful Holistic Therapy by Martin J Lara 1929831005Dokument5 SeitenUropathy The Most Powerful Holistic Therapy by Martin J Lara 1929831005parvesh sangwan100% (1)
- Medtech ReviewerDokument4 SeitenMedtech ReviewerLyudmyla Gillego100% (4)
- Health MateDokument3 SeitenHealth MateAnisah AquilaNoch keine Bewertungen
- Endodontic MicrobiologyDokument9 SeitenEndodontic MicrobiologySarah KahilNoch keine Bewertungen
- MLSP Midterm NotesDokument22 SeitenMLSP Midterm NotesKat JornadalNoch keine Bewertungen
- COPD LeafletDokument2 SeitenCOPD LeafletAN KnEeNoch keine Bewertungen
- Chapter2 - MEDICAL PERSONNEL PDFDokument39 SeitenChapter2 - MEDICAL PERSONNEL PDFRavi RajaNoch keine Bewertungen
- TOP 10 WI LD Foods: A Free Download FromDokument12 SeitenTOP 10 WI LD Foods: A Free Download Fromlifelonglearner1100% (3)
- 7057 24972 1 PBDokument133 Seiten7057 24972 1 PBDen NisNoch keine Bewertungen
- Around 2 Lakh May Have To Leave Kuwait: Minister Passes Buck To DGHSDokument12 SeitenAround 2 Lakh May Have To Leave Kuwait: Minister Passes Buck To DGHSshafikulNoch keine Bewertungen
- Bladder TumorDokument32 SeitenBladder TumorAngelynChristabellaNoch keine Bewertungen
- U2Dokument6 SeitenU2蔡維軒Noch keine Bewertungen
- Inflammatory Heart DiseaseDokument69 SeitenInflammatory Heart DiseaseLouise Anne Agnazata GayoNoch keine Bewertungen
- MUET Exercise 12 - Vocabulary W AnswerDokument8 SeitenMUET Exercise 12 - Vocabulary W AnswerIli Farhana100% (1)
- Detection of Brucella Species in ApparentlyDokument21 SeitenDetection of Brucella Species in ApparentlyHubdar Ali KolachiNoch keine Bewertungen
- MUDRASDokument5 SeitenMUDRASscsubbaraoNoch keine Bewertungen
- Vol19no8 PDF VersionDokument179 SeitenVol19no8 PDF VersionMark ReinhardtNoch keine Bewertungen
- Bio-Medical Waste ManagementDokument36 SeitenBio-Medical Waste Managementlyfzcool892097100% (6)
- Corneal Bacterial UlcerDokument48 SeitenCorneal Bacterial UlcerAkansha Rastogi100% (1)
- CHNDokument21 SeitenCHNCleo Gabiana Jubay100% (1)
- Non Enteric GIT PathogensDokument16 SeitenNon Enteric GIT PathogensMaria Cecilia FloresNoch keine Bewertungen
- Approach To Jaundice PatientDokument24 SeitenApproach To Jaundice Patientabela_amuluNoch keine Bewertungen
- Diagnostic MycologyDokument5 SeitenDiagnostic MycologyEarl de JesusNoch keine Bewertungen
- Sulfamethoxazole Trimethoprim PDFDokument10 SeitenSulfamethoxazole Trimethoprim PDFAsi SyyffaNoch keine Bewertungen
- 04 11 2016.tanzania National Guideline For Management Hiv and Aids May 2015. TaggedDokument290 Seiten04 11 2016.tanzania National Guideline For Management Hiv and Aids May 2015. TaggedArdilah Dwiagus SafitriNoch keine Bewertungen