Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Giardia BenchaidDokument2 SeitenGiardia BenchaidSaad MotawéaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Biological WeaponsDokument29 SeitenBiological WeaponsSaad Motawéa100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- 3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsDokument8 Seiten3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsSaad MotawéaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- 3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsDokument8 Seiten3-Bioelectrical Stimulation For People With Patterns Consistent With Certain Chronic InfectionsSaad MotawéaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Outbreak Investigation Monday's ExerciseDokument5 SeitenOutbreak Investigation Monday's ExerciseSaad MotawéaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- 20 - Outbreak Investigation ReportDokument26 Seiten20 - Outbreak Investigation ReportSaad Motawéa50% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- 2-Electrotherapy For Blood ElectrificationDokument12 Seiten2-Electrotherapy For Blood ElectrificationSaad MotawéaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Session 1 - BT Epi Response Training - Outbreak InvestigationDokument41 SeitenSession 1 - BT Epi Response Training - Outbreak InvestigationSaad MotawéaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Pathogenomic Research in Hungary Present Stage and PerspectivesDokument11 SeitenPathogenomic Research in Hungary Present Stage and PerspectivesSaad MotawéaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Julian Pe ToDokument41 SeitenJulian Pe ToSaad MotawéaNoch keine Bewertungen
- Parasites LectureDokument22 SeitenParasites LectureSaad MotawéaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Wong F Food OverviewDokument25 SeitenWong F Food OverviewSaad MotawéaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Common Intertinal Worms Found in Southern AfricaDokument100 SeitenCommon Intertinal Worms Found in Southern AfricaSaad MotawéaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- GM 05 TrypanosomDokument30 SeitenGM 05 TrypanosomSaad MotawéaNoch keine Bewertungen
- CasesDokument18 SeitenCasesSaad MotawéaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Paraneoplastic SyndromeDokument1 SeiteParaneoplastic SyndromeSaad MotawéaNoch keine Bewertungen
- Public Health Community Preparedness For SarsDokument29 SeitenPublic Health Community Preparedness For SarsSaad MotawéaNoch keine Bewertungen
- Case 2Dokument20 SeitenCase 2Saad MotawéaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- A Cute Appendic ItsDokument109 SeitenA Cute Appendic ItsYosevine Noviana PeranginanginNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Bizarre Claims of Hulda ClarkDokument16 SeitenThe Bizarre Claims of Hulda ClarkSaad Motawéa100% (1)
- Courses2006 2007Dokument8 SeitenCourses2006 2007Saad MotawéaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- S P - O F: Yllabus RE Rder ORMDokument1 SeiteS P - O F: Yllabus RE Rder ORMSaad MotawéaNoch keine Bewertungen
- New York University School of Medicine Meeting of The Curriculum CommitteeDokument2 SeitenNew York University School of Medicine Meeting of The Curriculum CommitteeSaad MotawéaNoch keine Bewertungen
- EpidemiologyDokument7 SeitenEpidemiologySaad MotawéaNoch keine Bewertungen
- Writing A ReferenceDokument1 SeiteWriting A ReferenceSaad MotawéaNoch keine Bewertungen
- ApplicationDokument11 SeitenApplicationSaad MotawéaNoch keine Bewertungen
- GuideDokument41 SeitenGuideSaad MotawéaNoch keine Bewertungen
- Annual Report 2005 PDFDokument54 SeitenAnnual Report 2005 PDFSaad MotawéaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Hexamine Fuel TabletDokument4 SeitenHexamine Fuel TabletSaad MotawéaNoch keine Bewertungen
- Supportive SupervisionDokument21 SeitenSupportive SupervisionSaad MotawéaNoch keine Bewertungen
- 2016 Vol 62 No - 2 - April May 2016 PDFDokument56 Seiten2016 Vol 62 No - 2 - April May 2016 PDFDanis Diba Sabatillah YaminNoch keine Bewertungen
- Abigail Domingo Physical AssessmentDokument87 SeitenAbigail Domingo Physical AssessmentVenus Maui RoqueNoch keine Bewertungen
- Tracheostomy Suctioning and HumidificationDokument5 SeitenTracheostomy Suctioning and HumidificationLucila LugoNoch keine Bewertungen
- Must Want Analysis - The FormDokument3 SeitenMust Want Analysis - The FormJohn NinoNoch keine Bewertungen
- Understanding Leukemia From A Lab PerspectiveDokument48 SeitenUnderstanding Leukemia From A Lab PerspectiveGlorya NathasiaNoch keine Bewertungen
- Ch02 Costing Out Nursing ServicesDokument26 SeitenCh02 Costing Out Nursing ServicesRicardo CanalesNoch keine Bewertungen
- Adl IadlDokument20 SeitenAdl IadlKrisna Eka Yudha100% (1)
- Bryan 3-24-17Dokument12 SeitenBryan 3-24-17Bryan VandentoornNoch keine Bewertungen
- Anatomy of The KidneyDokument7 SeitenAnatomy of The KidneyArgie Arguson IINoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Perspektif Pasien Dan Manajemen Tentang Mutu Pelayanan IGDDokument10 SeitenPerspektif Pasien Dan Manajemen Tentang Mutu Pelayanan IGDBenn TennNoch keine Bewertungen
- Diabetes MellitusDokument41 SeitenDiabetes MellitusYuttapol PimpisonNoch keine Bewertungen
- Comparison of UMN & LMN SyndromesDokument2 SeitenComparison of UMN & LMN SyndromesPJHGNoch keine Bewertungen
- Engel 1980 The Clinical Application of of The Biopsychosocial Model PDFDokument10 SeitenEngel 1980 The Clinical Application of of The Biopsychosocial Model PDFDiego Almanza HolguinNoch keine Bewertungen
- Service Delivary Organization Realignment: A Message From Karen Herd, Deputy Minister of Manitoba Health, Seniors and Active LivingDokument4 SeitenService Delivary Organization Realignment: A Message From Karen Herd, Deputy Minister of Manitoba Health, Seniors and Active LivingmatthewtrevithickNoch keine Bewertungen
- Clinical PatofisiologiDokument3 SeitenClinical PatofisiologiMuhammadLuthfi0% (2)
- Drug Interactions Results - MICROMEDEX®Dokument3 SeitenDrug Interactions Results - MICROMEDEX®Kike MenesesNoch keine Bewertungen
- Trauma From OcclusionDokument63 SeitenTrauma From OcclusionAvita RathNoch keine Bewertungen
- Quality of Nursing Care Provided For PreDokument16 SeitenQuality of Nursing Care Provided For PreAmmar Mustafa Mahadi AlzeinNoch keine Bewertungen
- Ocd Presentation 3Dokument11 SeitenOcd Presentation 3api-387888714Noch keine Bewertungen
- Secondary SurveyDokument2 SeitenSecondary SurveySakta SuryagunaNoch keine Bewertungen
- Care Giver Stress IndexDokument2 SeitenCare Giver Stress IndexcpradheepNoch keine Bewertungen
- A Case StudyDokument30 SeitenA Case StudyJie BandelariaNoch keine Bewertungen
- Body MechanicsDokument41 SeitenBody MechanicsPaul ReynaldoNoch keine Bewertungen
- Moses Cone Hospital MapDokument2 SeitenMoses Cone Hospital MapWfmy TegnaNoch keine Bewertungen
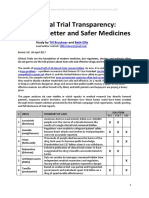
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Dokument21 SeitenClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerNoch keine Bewertungen
- Diagnosis of Adjustment Disorder Reliability of Its Clinical Use and Long-Term StabilityDokument6 SeitenDiagnosis of Adjustment Disorder Reliability of Its Clinical Use and Long-Term StabilitydmsdsNoch keine Bewertungen
- What Is Aerobic Exercise?Dokument2 SeitenWhat Is Aerobic Exercise?Diana BernalNoch keine Bewertungen
- Pengukuran Tekanan Darah Dan NadiDokument22 SeitenPengukuran Tekanan Darah Dan NadiBellaNoch keine Bewertungen
- MM Ous Microscan Eucast Gram Pos Ds 11 2013-01349656 PDFDokument2 SeitenMM Ous Microscan Eucast Gram Pos Ds 11 2013-01349656 PDFsazunaxNoch keine Bewertungen