Das könnte Ihnen auch gefallen
- Figo Staging CA EndometriumDokument9 SeitenFigo Staging CA Endometriumi305Noch keine Bewertungen
- Figo Staging CA EndometriumDokument9 SeitenFigo Staging CA Endometriumi305Noch keine Bewertungen
- Calcium and Vitamin D Intake and Risk of Incident Premenstrual SyndromeDokument7 SeitenCalcium and Vitamin D Intake and Risk of Incident Premenstrual Syndromei305Noch keine Bewertungen
- Agenesis VaginaDokument6 SeitenAgenesis Vaginai305Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- ANATOMY OF PIGEON (Columba Domestica)Dokument12 SeitenANATOMY OF PIGEON (Columba Domestica)Mellya RizkiNoch keine Bewertungen
- Dominance RelationshipsDokument30 SeitenDominance RelationshipsGretz AnticamaraNoch keine Bewertungen
- Breast Cancer KelseyDokument12 SeitenBreast Cancer Kelseyapi-3802092Noch keine Bewertungen
- MDG Women ChildDokument29 SeitenMDG Women ChildevleopoldNoch keine Bewertungen
- Corporate Documentary Two-Column Script: Human Life ServiceDokument8 SeitenCorporate Documentary Two-Column Script: Human Life ServicesuhastadasNoch keine Bewertungen
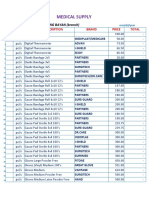
- Medical Supplies, & Baby Products PricelistDokument5 SeitenMedical Supplies, & Baby Products PricelistParmasya Ng Bayan Bacolor Main BranchNoch keine Bewertungen
- Reproductive System of SwineDokument11 SeitenReproductive System of SwineJaskhem LazoNoch keine Bewertungen
- Annotated BibliographyDokument11 SeitenAnnotated BibliographykjbjkNoch keine Bewertungen
- Lab Manual Animal Systematic II 2017 - Activity IDokument2 SeitenLab Manual Animal Systematic II 2017 - Activity IVio Indah BudiartiNoch keine Bewertungen
- Mutasi Gonosom ManusiaDokument20 SeitenMutasi Gonosom ManusiaMaharRkpNoch keine Bewertungen
- ART Bill 2021 POINTERDokument9 SeitenART Bill 2021 POINTERDURGESH DUBEYNoch keine Bewertungen
- Topic: 'Hiv and Aids'': Sub-Topic: Mode of TransmissionDokument16 SeitenTopic: 'Hiv and Aids'': Sub-Topic: Mode of TransmissionwesterNoch keine Bewertungen
- Https Teachingsexualhealth - Ca App Uploads Sites 4 DALP5-My-Period-Feb25Dokument10 SeitenHttps Teachingsexualhealth - Ca App Uploads Sites 4 DALP5-My-Period-Feb25Matthew ValenciaNoch keine Bewertungen
- Gestational Trophoblastic DiseaseDokument40 SeitenGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- 1 - Outline - Testosterone Levels in MenDokument5 Seiten1 - Outline - Testosterone Levels in MenJakeNoch keine Bewertungen
- Obgyn DOC373 Rev B Pages 637 726Dokument90 SeitenObgyn DOC373 Rev B Pages 637 726alodiarkNoch keine Bewertungen
- University of Limpopo School of Molecular and Life Sciences TestsDokument10 SeitenUniversity of Limpopo School of Molecular and Life Sciences TestsSjabuliso Madlala ThandekaNoch keine Bewertungen
- Sissy Forum2Dokument6 SeitenSissy Forum2Ali NasirNoch keine Bewertungen
- Treatment of Chlamydia Trachomatis InfectionDokument9 SeitenTreatment of Chlamydia Trachomatis InfectioneeeeewwwwwNoch keine Bewertungen
- Ayurvedic Medicine For Sex How To Increase Penis SizeDokument3 SeitenAyurvedic Medicine For Sex How To Increase Penis SizeZioAngel0% (1)
- General DataDokument6 SeitenGeneral DataGilbert Allen MateoNoch keine Bewertungen
- Reading-Comprehension Genetic Selection Answer KeyDokument4 SeitenReading-Comprehension Genetic Selection Answer KeyAngel Angeleri-priftis.Noch keine Bewertungen
- Oligomenoragia PDFDokument8 SeitenOligomenoragia PDFsjhfksglakdjalfsfNoch keine Bewertungen
- 12 Biology - Reproductive HealthDokument4 Seiten12 Biology - Reproductive HealthTanya Mishra100% (1)
- Full download Test Bank for Maternal Child Nursing Care With the Womens Health Companion Optimizing Outcomes for Mothers Children and Families 2nd Edition Susan l Ward Shelton m Hisley 665 1 pdf full chapterDokument35 SeitenFull download Test Bank for Maternal Child Nursing Care With the Womens Health Companion Optimizing Outcomes for Mothers Children and Families 2nd Edition Susan l Ward Shelton m Hisley 665 1 pdf full chaptertrigraph.loupingtaygv100% (20)
- Effects of Follicular and Luteal Phase Based Menstrual Cycle Resistance Training On Muscle Strength and MassDokument7 SeitenEffects of Follicular and Luteal Phase Based Menstrual Cycle Resistance Training On Muscle Strength and MassEmily ClarkNoch keine Bewertungen
- Copy-Induced Breeding in FishDokument31 SeitenCopy-Induced Breeding in Fishhafiz anasNoch keine Bewertungen
- Susunan AcaraDokument2 SeitenSusunan Acaraniko4eyesNoch keine Bewertungen
- Prenatal DevelopmentDokument29 SeitenPrenatal DevelopmentReymart MancaoNoch keine Bewertungen
- Newborn Essential Care PDFDokument54 SeitenNewborn Essential Care PDFMARK LENAND ESPIRITU100% (1)