Das könnte Ihnen auch gefallen
- THORACENTESISDokument14 SeitenTHORACENTESISKatherine Jeanne RosalNoch keine Bewertungen
- Checklist Thoracentesis (Charisse) ADokument6 SeitenChecklist Thoracentesis (Charisse) ARonel UsitaNoch keine Bewertungen
- ThoracentesisDokument9 SeitenThoracentesisPatricia G ChiuNoch keine Bewertungen
- Thoracentesis Is Also Known As Pleural Fluid AnalysisDokument3 SeitenThoracentesis Is Also Known As Pleural Fluid AnalysisJ.r. MercadoNoch keine Bewertungen
- ThoracentesisDokument12 SeitenThoracentesisAnusha Verghese0% (1)
- Thoracentesis ProDokument6 SeitenThoracentesis ProRaidis PangilinanNoch keine Bewertungen
- Thoracentesis: ProcedureDokument12 SeitenThoracentesis: Procedurealbert manievoNoch keine Bewertungen
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- NURSING CARE OF ADULTS II: Passbooks Study GuideVon EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNoch keine Bewertungen
- Med Surg Chapter 1Dokument2 SeitenMed Surg Chapter 1Judy072100% (1)
- Interactive Quiz: Deal or No DealDokument7 SeitenInteractive Quiz: Deal or No DealShaira Jean GeminaNoch keine Bewertungen
- Chest Tube ModuleDokument37 SeitenChest Tube ModuleEdison Reyes100% (1)
- ECG Reading & InterpretationDokument52 SeitenECG Reading & InterpretationRoy Francis B. CaspeNoch keine Bewertungen
- Group 5 - Hemodialysis - Chronic Kidney FailureDokument31 SeitenGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraNoch keine Bewertungen
- Chapter 2 SampleDokument38 SeitenChapter 2 SampleLospa Stocazzo100% (1)
- Fundamentals Modules 1-10 Study GuidesDokument278 SeitenFundamentals Modules 1-10 Study GuidesNurseAmy100% (1)
- Assessment of The Thorax and Lungs 2014Dokument9 SeitenAssessment of The Thorax and Lungs 2014alphabennydelta4468Noch keine Bewertungen
- Icu Equipments BY: Presented Bhupender Kumar MehtoDokument35 SeitenIcu Equipments BY: Presented Bhupender Kumar Mehtobhupendermehto012Noch keine Bewertungen
- M.SC Nursing Syllabus Revised 2018 - 19-23082019-1Dokument344 SeitenM.SC Nursing Syllabus Revised 2018 - 19-23082019-1Divya ToppoNoch keine Bewertungen
- 18 NCP Ileal ConduitDokument11 Seiten18 NCP Ileal ConduitICa MarlinaNoch keine Bewertungen
- M Digestion" Absorption" EliminationDokument104 SeitenM Digestion" Absorption" EliminationChristine Carol FilipinasNoch keine Bewertungen
- Physical Assessment (Ippa)Dokument14 SeitenPhysical Assessment (Ippa)Barbara HsuNoch keine Bewertungen
- Nursing Informatics: de Lara, Denise Dominique M. Quiamco, Precious Diane S. RNDokument113 SeitenNursing Informatics: de Lara, Denise Dominique M. Quiamco, Precious Diane S. RNPrecious Diane QuiamcoNoch keine Bewertungen
- Nursing Management in Abdominal SurgeryDokument19 SeitenNursing Management in Abdominal Surgeryejguy7777100% (2)
- Perioperative Nursing CareDokument47 SeitenPerioperative Nursing CareTessa Bagus AriyantoNoch keine Bewertungen
- Nursing Care of Clients With Upper Gastrointestinal Disorder 1Dokument149 SeitenNursing Care of Clients With Upper Gastrointestinal Disorder 1Andrea TylerNoch keine Bewertungen
- Naso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringDokument12 SeitenNaso Orogastric Tube Guideline For The Care of Neonate Child or Young Person RequiringmeisygraniaNoch keine Bewertungen
- Care of Pediatric Client With Dermatologic DisorderDokument3 SeitenCare of Pediatric Client With Dermatologic DisorderAraw GabiNoch keine Bewertungen
- Fundamentals of Nursing 1Dokument6 SeitenFundamentals of Nursing 1Ruel M. BersabeNoch keine Bewertungen
- Case Study PeriopDokument3 SeitenCase Study PeriopSteve25% (4)
- Pharamacology Notes 3Dokument7 SeitenPharamacology Notes 3Martinet CalvertNoch keine Bewertungen
- Assessment of Respiratory Function Chpt.20Dokument32 SeitenAssessment of Respiratory Function Chpt.20Maricar RosasNoch keine Bewertungen
- Medication Administration - Parenteral RouteDokument3 SeitenMedication Administration - Parenteral RouteRhiz Antonio67% (3)
- GROUP 3 - CASE STUDY - TraumaDokument5 SeitenGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNoch keine Bewertungen
- Nursing ReviewerDokument10 SeitenNursing ReviewerChristine Hernandez100% (1)
- Patient Position PDFDokument60 SeitenPatient Position PDFDana RoxanaNoch keine Bewertungen
- Medical Surgical NursingDokument66 SeitenMedical Surgical Nursing04eden100% (3)
- 2022 Level 4 Intravenous TherapyDokument65 Seiten2022 Level 4 Intravenous TherapyBokNoch keine Bewertungen
- Cardiac SurgeryDokument35 SeitenCardiac SurgeryxxxNoch keine Bewertungen
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDokument2 SeitenPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenNoch keine Bewertungen
- Ethico Legal of Perioperative NursingDokument19 SeitenEthico Legal of Perioperative NursingAziil Liiza100% (1)
- ABC Dictionary of Urinary SystemDokument26 SeitenABC Dictionary of Urinary Systemaby_romero9750% (2)
- ChestTubes CareDokument21 SeitenChestTubes CareAnusha VergheseNoch keine Bewertungen
- Management of Arterial LineDokument16 SeitenManagement of Arterial LineFarcasanu Liana GeorgianaNoch keine Bewertungen
- Tracheostomy CareDokument22 SeitenTracheostomy CareHollan Galicia100% (1)
- CATHETERIZATIONDokument13 SeitenCATHETERIZATIONSarah Uy Caronan100% (1)
- Example of Nursing Care Plan (Pathophysiology)Dokument5 SeitenExample of Nursing Care Plan (Pathophysiology)Elizabeth ZamoraNoch keine Bewertungen
- Community Health Nursing Notes (Second Year)Dokument6 SeitenCommunity Health Nursing Notes (Second Year)anette katrinNoch keine Bewertungen
- ThoracentesisDokument4 SeitenThoracentesisDunathree Caranto CorcueraNoch keine Bewertungen
- Patient Positioning in Operating TheatreDokument52 SeitenPatient Positioning in Operating TheatreFatkhul AdhiatmadjaNoch keine Bewertungen
- NCM 212 - Pharmacokinetics and PharmacodynamicsDokument11 SeitenNCM 212 - Pharmacokinetics and PharmacodynamicsLYRIZZA LEA BHEA DESIATANoch keine Bewertungen
- HEC BSN 4 YearDokument254 SeitenHEC BSN 4 Yearkhizar hayatNoch keine Bewertungen
- Medical PrefixesDokument6 SeitenMedical PrefixesNasirah Nasi ImpitNoch keine Bewertungen
- Pleural Fluid Analysis: How The Test Is PerformedDokument4 SeitenPleural Fluid Analysis: How The Test Is PerformedKevin LlorenteNoch keine Bewertungen
- Periop Power PointDokument97 SeitenPeriop Power PointAldrine Albor Anyayahan INoch keine Bewertungen
- ChesttubedrainageDokument65 SeitenChesttubedrainagejerinthomasrajanNoch keine Bewertungen
- Digestive SystemDokument117 SeitenDigestive SystemKBDNoch keine Bewertungen
- Thoracentesis IntroductionDokument8 SeitenThoracentesis Introductionjyoti singhNoch keine Bewertungen
- SP42 Thoracentesis (Adult)Dokument7 SeitenSP42 Thoracentesis (Adult)Adam HuzaibyNoch keine Bewertungen
- Synthetic Approach ReportDokument20 SeitenSynthetic Approach ReportMarivic Diano100% (1)
- Return On InvestmentDokument15 SeitenReturn On InvestmentMarivic DianoNoch keine Bewertungen
- Wellness PowerpointDokument28 SeitenWellness PowerpointMarivic Diano0% (1)
- Light of HOPEDokument33 SeitenLight of HOPEMarivic DianoNoch keine Bewertungen
- BiologyDokument42 SeitenBiologyMarivic DianoNoch keine Bewertungen
- Why Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Dokument2 SeitenWhy Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Marivic DianoNoch keine Bewertungen
- Animal Tissues: Asia Technological School of Science and ArtsDokument2 SeitenAnimal Tissues: Asia Technological School of Science and ArtsMarivic DianoNoch keine Bewertungen
- Under The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsDokument79 SeitenUnder The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsMarivic DianoNoch keine Bewertungen
- Hospital Incident Command System (HICS) : Reported byDokument42 SeitenHospital Incident Command System (HICS) : Reported byMarivic DianoNoch keine Bewertungen
- Iv Regulation and Controlling DevicesDokument21 SeitenIv Regulation and Controlling DevicesMarivic DianoNoch keine Bewertungen
- Nurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsDokument31 SeitenNurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsMarivic Diano100% (1)
- Nurse To Colleagues: You Deserve A Break Today: by Tyler SmithDokument2 SeitenNurse To Colleagues: You Deserve A Break Today: by Tyler SmithMarivic DianoNoch keine Bewertungen
- Anatomy and Physiology of BVDokument16 SeitenAnatomy and Physiology of BVMarivic DianoNoch keine Bewertungen
- Suprising Truths About MotivationDokument2 SeitenSuprising Truths About MotivationMarivic DianoNoch keine Bewertungen
- Disaster Risk Management and MitigationDokument5 SeitenDisaster Risk Management and MitigationMarivic DianoNoch keine Bewertungen
- Fractures: (On Which We Will Likely Be Pimped)Dokument66 SeitenFractures: (On Which We Will Likely Be Pimped)Marivic DianoNoch keine Bewertungen
- Renal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyDokument50 SeitenRenal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyMarivic DianoNoch keine Bewertungen
- MeaslesDokument11 SeitenMeaslesMarivic DianoNoch keine Bewertungen
- Palliative and Terminal CareDokument78 SeitenPalliative and Terminal CareMarivic DianoNoch keine Bewertungen
- Fluid and Electrolytes Report!!Dokument20 SeitenFluid and Electrolytes Report!!Marivic DianoNoch keine Bewertungen
- Applied Clinical Anatomy: The Successful Integration of Anatomy Into Specialty-Specific Senior ElectivesDokument13 SeitenApplied Clinical Anatomy: The Successful Integration of Anatomy Into Specialty-Specific Senior ElectivesHesti AnwarNoch keine Bewertungen
- Department of Surgery Common ICD and RUVDokument2 SeitenDepartment of Surgery Common ICD and RUVAnne Lorraine BringasNoch keine Bewertungen
- NP3 Nursing Board Exam June 2007Dokument44 SeitenNP3 Nursing Board Exam June 2007rem_cen24100% (1)
- Pleural EffusionDokument2 SeitenPleural EffusionKhalid Mahmud Arifin100% (1)
- EmpyemaDokument33 SeitenEmpyemavirz23100% (1)
- Medical Surgical Nursing TionkoDokument40 SeitenMedical Surgical Nursing TionkojeshemaNoch keine Bewertungen
- Aspiration PneumoniaDokument16 SeitenAspiration PneumoniaFeni DianiNoch keine Bewertungen
- Blue Protocol. Lung Ultrasound in The Critically IllDokument12 SeitenBlue Protocol. Lung Ultrasound in The Critically IllRomina Alfonsina Decap CarrascoNoch keine Bewertungen
- Chest Tubes and ThoracentesisDokument18 SeitenChest Tubes and ThoracentesisecleptosNoch keine Bewertungen
- Pleural EffusionDokument34 SeitenPleural EffusionFazlullah HashmiNoch keine Bewertungen
- 'Batangas Medical Center Case Report by PGI Carlos H. AcuñaDokument7 Seiten'Batangas Medical Center Case Report by PGI Carlos H. AcuñaCarlos H. AcuñaNoch keine Bewertungen
- Sample Review Questions in Medical and Surgical Nursing and Sample Board Exam QuestionsDokument22 SeitenSample Review Questions in Medical and Surgical Nursing and Sample Board Exam Questionstinea nigraNoch keine Bewertungen
- 3.pleural Effusion Imaging - Overview, Radiography, Computed TomographyDokument32 Seiten3.pleural Effusion Imaging - Overview, Radiography, Computed TomographyAchmadRizaNoch keine Bewertungen
- 5 MED II 1 - PneumoniaDokument11 Seiten5 MED II 1 - PneumoniaDeann RoscomNoch keine Bewertungen
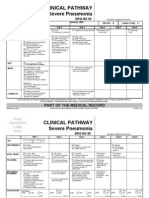
- Clinical Pathways Severe PneumoniaDokument2 SeitenClinical Pathways Severe PneumoniaaandakuNoch keine Bewertungen
- krok 2 З English 2007 2020 SURGERY+Dokument79 Seitenkrok 2 З English 2007 2020 SURGERY+Zeynep YılmaztürkNoch keine Bewertungen
- Approach To Pleural EffusionDokument46 SeitenApproach To Pleural EffusionBaskoro Tri LaksonoNoch keine Bewertungen
- Nursing Assignment 2Dokument12 SeitenNursing Assignment 2ticticNoch keine Bewertungen
- Surgery & Pediatrics SurgeryDokument111 SeitenSurgery & Pediatrics SurgeryHIMANSHU GUPTANoch keine Bewertungen
- Important Numbers For SMLEDokument3 SeitenImportant Numbers For SMLEAkpevwe EmefeNoch keine Bewertungen
- Bullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Dokument15 SeitenBullets: "Victory Belongs To Those Who Are Most Persevering. Ad Majorem Dei Gloriam."Jhaylord mendozaNoch keine Bewertungen
- Prioritization, Delegation & Assignment 1-3Dokument12 SeitenPrioritization, Delegation & Assignment 1-3eric100% (2)
- Test Bank Clinical Manifestations and Assessment of Respiratory Disease Mid PartDokument24 SeitenTest Bank Clinical Manifestations and Assessment of Respiratory Disease Mid Partweekup035Noch keine Bewertungen
- Ecografia Toracica PDFDokument12 SeitenEcografia Toracica PDFCristinaLucanNoch keine Bewertungen
- filePV 31 05 232Dokument11 SeitenfilePV 31 05 232Raul Hernandez SotoNoch keine Bewertungen
- Oxygen InsuffiencyDokument21 SeitenOxygen InsuffiencyAntony Raj Culandai Swamy100% (1)
- Pathophysiology Plueral Effusion Secondary To Pneumonia: GreenDokument7 SeitenPathophysiology Plueral Effusion Secondary To Pneumonia: Greenkuro hanabusaNoch keine Bewertungen
- Report EmpyemaDokument32 SeitenReport EmpyemaMylah CruzNoch keine Bewertungen
- Thoracentesis IntroductionDokument8 SeitenThoracentesis Introductionjyoti singhNoch keine Bewertungen