Das könnte Ihnen auch gefallen
- Nutritional AssesmentDokument58 SeitenNutritional AssesmentመክትNoch keine Bewertungen
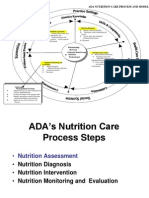
- Nutrition Care ProcessDokument48 SeitenNutrition Care ProcessNariNoch keine Bewertungen
- Nutritional Assessment Lecture 1Dokument28 SeitenNutritional Assessment Lecture 1ESUFIYAN ALWSABINoch keine Bewertungen
- Nutrition Care Process (ADIME Process)Dokument15 SeitenNutrition Care Process (ADIME Process)Eizel Nhey G. JADENoch keine Bewertungen
- Nutrition Care Process (NCP)Dokument48 SeitenNutrition Care Process (NCP)annyeong_123100% (1)
- Trespasso SdhsDokument13 SeitenTrespasso SdhsRacquel Jahn CorderoNoch keine Bewertungen
- Nutrition AssessmentDokument32 SeitenNutrition AssessmentJobelyn MalisaNoch keine Bewertungen
- NCP Assessment Diagnosis Intervention p1 PDF NCPLecDokument67 SeitenNCP Assessment Diagnosis Intervention p1 PDF NCPLecJennie ManobanNoch keine Bewertungen
- Nutrition Care Process Briefer CP OrientationDokument37 SeitenNutrition Care Process Briefer CP OrientationDadanNoch keine Bewertungen
- Chap1 Introduction To Nutritional AssessmentDokument32 SeitenChap1 Introduction To Nutritional AssessmentAbdi Khalaq Ali Hashi100% (1)
- Nutritional RequirementsDokument56 SeitenNutritional Requirementsashenafihailemariam43Noch keine Bewertungen
- Pediatric Nutrition 2020 SGDokument27 SeitenPediatric Nutrition 2020 SGHajira GhaniNoch keine Bewertungen
- AnthropometryDokument75 SeitenAnthropometryAsad AliNoch keine Bewertungen
- (Riazuddin)Dokument14 Seiten(Riazuddin)Mohona Rahman KhanNoch keine Bewertungen
- Chap 1Dokument41 SeitenChap 1vchan318Noch keine Bewertungen
- Planning A Healthy Diet - 1 & 2 (2) .PPT 12343Dokument53 SeitenPlanning A Healthy Diet - 1 & 2 (2) .PPT 12343Jrose CuerpoNoch keine Bewertungen
- Planning A Healthy Diet - 1 & 2Dokument50 SeitenPlanning A Healthy Diet - 1 & 2Angie MandeoyaNoch keine Bewertungen
- SHS 406 Lec-03Dokument67 SeitenSHS 406 Lec-03Shahzad MazharNoch keine Bewertungen
- Nutritional AssessmentDokument28 SeitenNutritional AssessmentArella Flores100% (1)
- Assessment of The Nutritional Status of The CommunityDokument29 SeitenAssessment of The Nutritional Status of The CommunitySarad Chand YadavNoch keine Bewertungen
- Planning A Healthy Diet - 1 & 2Dokument49 SeitenPlanning A Healthy Diet - 1 & 2Carol Neng CalupitanNoch keine Bewertungen
- NDT Complete Midterm Lecture 3Dokument88 SeitenNDT Complete Midterm Lecture 3nicolediazNoch keine Bewertungen
- The Tools of Nutrition AssessmentDokument12 SeitenThe Tools of Nutrition AssessmentJaash De Guzman50% (2)
- Dietary Reference IntakesDokument22 SeitenDietary Reference Intakeschicklet escalonaNoch keine Bewertungen
- NCP 1 Na-SnapDokument1 SeiteNCP 1 Na-SnapAlvia ArvenaNoch keine Bewertungen
- Dietary AssessmentDokument20 SeitenDietary AssessmentharviliaNoch keine Bewertungen
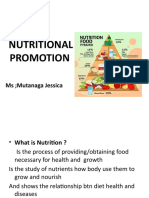
- Nutritional Promotion: Ms Mutanaga JessicaDokument22 SeitenNutritional Promotion: Ms Mutanaga JessicaJesca MutanagaNoch keine Bewertungen
- AnthroDokument12 SeitenAnthroBea ArrezaNoch keine Bewertungen
- 3Dokument13 Seiten3Statistician Tijani IsihaqNoch keine Bewertungen
- Nutrition Assessment 1Dokument22 SeitenNutrition Assessment 1KHALEEL SALEHNoch keine Bewertungen
- 3.A Diet Management of DiabetesDokument22 Seiten3.A Diet Management of DiabetesNixon KeyaNoch keine Bewertungen
- 2nutritionassmt Studay1819Dokument101 Seiten2nutritionassmt Studay1819RaysonChoo100% (2)
- Lesson 3 Nutritional AssessmentDokument84 SeitenLesson 3 Nutritional AssessmentJake ArizapaNoch keine Bewertungen
- Assessment of Nutritional StatusDokument16 SeitenAssessment of Nutritional StatusJaspreet SinghNoch keine Bewertungen
- Nutrition Assesment OverviewDokument5 SeitenNutrition Assesment OverviewDea MustikaNoch keine Bewertungen
- Assessment of Nutritional StatusDokument38 SeitenAssessment of Nutritional Statusmichael jan de celis100% (3)
- Nutrition Care ProcessDokument22 SeitenNutrition Care ProcessIrhamna Fauziah100% (1)
- Kuliah Gizi Klinik Dasar 1Dokument59 SeitenKuliah Gizi Klinik Dasar 1yuliaNoch keine Bewertungen
- Lec1 Fall23 FSC520 Nutri Assess IntroDokument35 SeitenLec1 Fall23 FSC520 Nutri Assess IntroFatma ZamanNoch keine Bewertungen
- Nutritional Assessment of Individuals: To Prepare A Nutrition Assessment, A Trained Health-Care Professional UsesDokument15 SeitenNutritional Assessment of Individuals: To Prepare A Nutrition Assessment, A Trained Health-Care Professional Usesmedical studiesNoch keine Bewertungen
- Food Choices and Human HealthDokument60 SeitenFood Choices and Human HealthMohamed SamaheejiNoch keine Bewertungen
- Nutritional Assessment: A. Yasmin Syauki Nutrition Department School of Medicine Hasanuddin UniversityDokument47 SeitenNutritional Assessment: A. Yasmin Syauki Nutrition Department School of Medicine Hasanuddin UniversitylindaNoch keine Bewertungen
- Process Nutrition Care Terminology (NCPT) : R GHTDokument64 SeitenProcess Nutrition Care Terminology (NCPT) : R GHTnoviananurhanifahNoch keine Bewertungen
- CH 01 PPT LectureDokument52 SeitenCH 01 PPT LectureCarlos Funs100% (1)
- Nutritional AssessmentDokument5 SeitenNutritional AssessmentimnasNoch keine Bewertungen
- 2019 AM Functional Nutrition Assessment Presentation StrangeDokument61 Seiten2019 AM Functional Nutrition Assessment Presentation StrangeYasminNoch keine Bewertungen
- Nutritional AssessmentDokument8 SeitenNutritional AssessmentShaimaa Emad100% (1)
- 1 Nutrition IN Health and Illness 1Dokument41 Seiten1 Nutrition IN Health and Illness 1Worku KifleNoch keine Bewertungen
- Comprehensive Geriatric Assessment (CGA) / Pengkajian: Paripurna Pasien Geriatri (P3G)Dokument55 SeitenComprehensive Geriatric Assessment (CGA) / Pengkajian: Paripurna Pasien Geriatri (P3G)Ichtiarsyah SuminarNoch keine Bewertungen
- Chapter1 With VoiceDokument40 SeitenChapter1 With VoiceLiraNoch keine Bewertungen
- 5as Powerpoint PresentationDokument50 Seiten5as Powerpoint Presentationkahtrsh100% (1)
- Nutrition Assessment ResourcesDokument2 SeitenNutrition Assessment ResourcesAnna DrakeNoch keine Bewertungen
- Chapter 2: Tools For Designing A Healthy DietDokument46 SeitenChapter 2: Tools For Designing A Healthy DietRichard Gelman0% (1)
- NCPT For EALDokument61 SeitenNCPT For EALAsri SubarjatiNoch keine Bewertungen
- AttachmentDokument34 SeitenAttachmentBp hoNoch keine Bewertungen
- NCP Eal 201711 PDFDokument64 SeitenNCP Eal 201711 PDFAnisaNoch keine Bewertungen
- PEM Growth AssessmentDokument8 SeitenPEM Growth AssessmentRavikumar ChodavarapuNoch keine Bewertungen
- Dietary Planning, Canada's Food Guide and Nutritional RequirementsDokument8 SeitenDietary Planning, Canada's Food Guide and Nutritional RequirementsSar PattsNoch keine Bewertungen
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionVon EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionNoch keine Bewertungen
- The Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingVon EverandThe Non-Diet Approach Guidebook for Dietitians (2013): A how-to guide for applying the Non-Diet Approach to Individualised Dietetic CounsellingNoch keine Bewertungen
- The Problem and Its Scope: Encyclopedia of Food Sciences and Nutrition (Second EditionDokument39 SeitenThe Problem and Its Scope: Encyclopedia of Food Sciences and Nutrition (Second EditionEvogen GenesisNoch keine Bewertungen
- FBB PracticalproteinguideDokument73 SeitenFBB PracticalproteinguideRohit Yadav80% (5)
- Total Parenteral Nutrition: Presented byDokument46 SeitenTotal Parenteral Nutrition: Presented byMuhammad YamnainNoch keine Bewertungen
- Juvenile Cat Altriciality Survival: Kitoun Chitoun ChetonDokument5 SeitenJuvenile Cat Altriciality Survival: Kitoun Chitoun ChetonseanNoch keine Bewertungen
- Obesity Project 2021Dokument16 SeitenObesity Project 2021JIESSNU A/L ANBARASU MoeNoch keine Bewertungen
- Diabetes AdimeDokument3 SeitenDiabetes Adimeapi-330880468100% (3)
- Unit 5Dokument9 SeitenUnit 5Mai TrinhNoch keine Bewertungen
- Eating A Balanced DietDokument3 SeitenEating A Balanced DietmarinahuamaniNoch keine Bewertungen
- Calorie and Macro Calculator 1Dokument8 SeitenCalorie and Macro Calculator 1Monal SinghNoch keine Bewertungen
- Seven Steps To A Healthy, Fit, Age-Resistant BodyDokument359 SeitenSeven Steps To A Healthy, Fit, Age-Resistant BodyMeschinohealthNoch keine Bewertungen
- FAO - 2008 - Updating The Minimum Dietary Energy RequirementsDokument16 SeitenFAO - 2008 - Updating The Minimum Dietary Energy RequirementssousaribeirojuniorNoch keine Bewertungen
- Semi Detailed Lesson Plan in Tle 10 4th QuarterDokument5 SeitenSemi Detailed Lesson Plan in Tle 10 4th Quarterleslie oblendaNoch keine Bewertungen
- Community Nutrition Program Plan PowerpointDokument20 SeitenCommunity Nutrition Program Plan Powerpointapi-523266509Noch keine Bewertungen
- Teds 2013 Nutra Clear NT Ultra SsDokument2 SeitenTeds 2013 Nutra Clear NT Ultra Ssapi-226773621Noch keine Bewertungen
- Path-Fit 1 Activity Answer SheetDokument1 SeitePath-Fit 1 Activity Answer SheetCalo, Loren D.Noch keine Bewertungen
- Text Which Foods Are Toxic To Cats and DogsDokument2 SeitenText Which Foods Are Toxic To Cats and Dogsjosmar valencia IslasNoch keine Bewertungen
- Grade 7. Unit 5 - Vietnamese Food and Drink Practice 3. Consolidation I. Find The Word Which Has A Different Sound in The Part UnderlineDokument7 SeitenGrade 7. Unit 5 - Vietnamese Food and Drink Practice 3. Consolidation I. Find The Word Which Has A Different Sound in The Part Underlineclone cypherwolfNoch keine Bewertungen
- HealthifyPro Information CollateralDokument11 SeitenHealthifyPro Information CollateralMaheshwar ReddyNoch keine Bewertungen
- Cognitive VitalityDokument80 SeitenCognitive VitalitySamscribding100% (1)
- Black Soldier Fly Defatted Meal As A Dietary Protein Source For Broiler Chickens: Effects On Carcass Traits, Breast Meat Quality and SafetyDokument9 SeitenBlack Soldier Fly Defatted Meal As A Dietary Protein Source For Broiler Chickens: Effects On Carcass Traits, Breast Meat Quality and SafetyThe Awesome RBNoch keine Bewertungen
- Diabetes Reversal PlanDokument7 SeitenDiabetes Reversal PlanMohammed ShazebNoch keine Bewertungen
- Baru AlmondDokument6 SeitenBaru AlmondmajabulatNoch keine Bewertungen
- HTS Nutrition GuideDokument28 SeitenHTS Nutrition GuideNoel MartinNoch keine Bewertungen
- 9 Nutrition Rules For Building MuscleDokument1 Seite9 Nutrition Rules For Building MuscleJeremiahgibsonNoch keine Bewertungen
- Taxofit® Joints Plus Chrono Depot - KlosterfrauDokument2 SeitenTaxofit® Joints Plus Chrono Depot - KlosterfrauDušan JovanovićNoch keine Bewertungen
- Stop COVID (19) Cold - Dr. Mercola 2020Dokument17 SeitenStop COVID (19) Cold - Dr. Mercola 2020petr18Noch keine Bewertungen
- Pediatric Helpful HintsDokument32 SeitenPediatric Helpful Hintspainah sumodiharjoNoch keine Bewertungen
- OPTplus Guidelines RevGB 12janrevfebDokument81 SeitenOPTplus Guidelines RevGB 12janrevfebmynoytech80% (5)
- Guidelines ASPENDokument138 SeitenGuidelines ASPENJaqueline Odair100% (1)
- Insights Mindmap Assignment ExampleDokument3 SeitenInsights Mindmap Assignment ExamplejosswayarmylopNoch keine Bewertungen