Das könnte Ihnen auch gefallen
- GIT OverviewDokument108 SeitenGIT OverviewNasser SalahNoch keine Bewertungen
- Non Variceal Upper GI Bleeding: Causes, Risk Factors, Diagnosis and ManagementDokument66 SeitenNon Variceal Upper GI Bleeding: Causes, Risk Factors, Diagnosis and ManagementsarangpbNoch keine Bewertungen
- Disturbances in Ingestion: Prepared By: Jan Paul Valeros Sicat, PHRN, USRNDokument41 SeitenDisturbances in Ingestion: Prepared By: Jan Paul Valeros Sicat, PHRN, USRNAriane-Gay Cristobal Duran100% (1)
- Update On The Management of PancreatitisDokument92 SeitenUpdate On The Management of Pancreatitisadamu mohammadNoch keine Bewertungen
- ICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomDokument3 SeitenICD 10.0: K29 Condition/Disease: Gastritis Description:: SymptomvicndubNoch keine Bewertungen
- Acute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetDokument40 SeitenAcute Pancreatitis: Sudden Severe Abdominal Pain Systemic UpsetcoolcaesarNoch keine Bewertungen
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDokument33 SeitenDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiNoch keine Bewertungen
- Acute Pancreatitis GuideDokument100 SeitenAcute Pancreatitis GuideJu Lie AnnNoch keine Bewertungen
- Acid Peptic Disorders The Spotlight Is On!Dokument41 SeitenAcid Peptic Disorders The Spotlight Is On!Wally HoneyNoch keine Bewertungen
- Liver D PDFDokument71 SeitenLiver D PDFermichoNoch keine Bewertungen
- Exmd 509 Mcgill Stomach 2016Dokument36 SeitenExmd 509 Mcgill Stomach 2016Sora OhNoch keine Bewertungen
- PepticDokument29 SeitenPepticMuhammad Irfan JamilNoch keine Bewertungen
- Acute PancreatitisDokument11 SeitenAcute Pancreatitispeter_soósNoch keine Bewertungen
- Peptis Ulcer-Bs TâmDokument27 SeitenPeptis Ulcer-Bs TâmÁnh PhạmNoch keine Bewertungen
- PankreatitisDokument107 SeitenPankreatitisIlmiah BagusNoch keine Bewertungen
- Cholelithiasis and CholecystitisDokument28 SeitenCholelithiasis and Cholecystitisandreva8Noch keine Bewertungen
- Gatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Dokument62 SeitenGatot Sugiharto, MD, Internist Faculty of Medicine, UWKS Lecture - 2010Ardi PratamaNoch keine Bewertungen
- Pancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)Dokument6 SeitenPancreatitis: Pancreatitis Is Inflammation of The Pancreas. It Occurs When Pancreatic Enzymes (Especially Trypsin)tianallyNoch keine Bewertungen
- Lecture 1part 2Dokument50 SeitenLecture 1part 2mashe1Noch keine Bewertungen
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Dokument46 SeitenJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Edwin Jose SNoch keine Bewertungen
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDokument82 SeitenGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- Peptic Ulcer Disease: Erwin Budi CahyonoDokument29 SeitenPeptic Ulcer Disease: Erwin Budi Cahyonoshavira nuzulaNoch keine Bewertungen
- Everything You Need to Know About Peptic Ulcer DiseaseDokument29 SeitenEverything You Need to Know About Peptic Ulcer Diseasehanizah kurniaNoch keine Bewertungen
- Clinical Clerk Seminar Series: Approach To Gi BleedsDokument11 SeitenClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388Noch keine Bewertungen
- Abd PainDokument35 SeitenAbd PainHandrian RahmanNoch keine Bewertungen
- Based on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDokument37 SeitenBased on the information provided, the most likely causative organism is Cytomegalovirus (CMV). CMV is a common opportunistic infection in HIV/AIDS patients that can cause esophageal ulcersDanielle FosterNoch keine Bewertungen
- Bile, Bile Duct and Pancreatic DiseaseDokument82 SeitenBile, Bile Duct and Pancreatic Diseaseshahrul rahmanNoch keine Bewertungen
- Peptic Ulcer DiseaseDokument2 SeitenPeptic Ulcer DiseaseAlexander EnnesNoch keine Bewertungen
- Peptic Ulcer Disease (PUD) : Symptomatology (Common)Dokument12 SeitenPeptic Ulcer Disease (PUD) : Symptomatology (Common)Asni LongaNoch keine Bewertungen
- Topics in Gastroenterology - 2014Dokument79 SeitenTopics in Gastroenterology - 2014BwatNoch keine Bewertungen
- Peptic Ulcer Disease: "Something Is Eating at Me"Dokument37 SeitenPeptic Ulcer Disease: "Something Is Eating at Me"bobtaguba100% (1)
- "Belajar Mandiri 2.4.2" Penyakit Inslamasi Pada Saluran CernaDokument73 Seiten"Belajar Mandiri 2.4.2" Penyakit Inslamasi Pada Saluran CernaNununNoch keine Bewertungen
- Peptic Ulcer DiseaseDokument98 SeitenPeptic Ulcer DiseaseOmar MohammedNoch keine Bewertungen
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDokument18 SeitenEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanNoch keine Bewertungen
- Curs 2-3 2023Dokument115 SeitenCurs 2-3 2023Andreea GuraliucNoch keine Bewertungen
- Biliary Tract Dis Pancreatitis 2015Dokument143 SeitenBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNoch keine Bewertungen
- Acute Pancreatitis Guide: Causes, Symptoms, TreatmentDokument100 SeitenAcute Pancreatitis Guide: Causes, Symptoms, TreatmentabelNoch keine Bewertungen
- Peptic Ulcer DiseaseDokument119 SeitenPeptic Ulcer DiseaseJoy LacunaNoch keine Bewertungen
- GI BleedDokument28 SeitenGI BleedAnn Lan100% (1)
- Peptic Ulcer DiseaseDokument45 SeitenPeptic Ulcer DiseaseChinna ChadayanNoch keine Bewertungen
- Pancreas and GITDokument21 SeitenPancreas and GITAbuzarNoch keine Bewertungen
- GIN L9 Shabot 0708Dokument53 SeitenGIN L9 Shabot 0708api-3799874Noch keine Bewertungen
- Lower GI BleedingDokument40 SeitenLower GI BleedingMohammad Firdaus100% (2)
- 4-Hepatobiliary DiseaseDokument22 Seiten4-Hepatobiliary Diseaseabdalmajeed alshammaryNoch keine Bewertungen
- Gastrointestinal Emergencies in Children: Magdalena Trzepizur, MDDokument64 SeitenGastrointestinal Emergencies in Children: Magdalena Trzepizur, MDlindaNoch keine Bewertungen
- By DR.: Haitham Mokhtar Mohamed Abd AllahDokument101 SeitenBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyNoch keine Bewertungen
- GI Stomach PDFDokument65 SeitenGI Stomach PDFBatool SherbiniNoch keine Bewertungen
- Definition and Etiology: PancreatitisDokument24 SeitenDefinition and Etiology: PancreatitisAliyah Tofani PawelloiNoch keine Bewertungen
- Gastro 2006Dokument66 SeitenGastro 2006Nyoman TapayanaNoch keine Bewertungen
- Fever and Abdominal Pain - Causes and DiagnosisDokument7 SeitenFever and Abdominal Pain - Causes and DiagnosisgianneNoch keine Bewertungen
- Acute PancreatitisDokument64 SeitenAcute PancreatitisOleksandr RotarNoch keine Bewertungen
- Approach To JaundiceDokument36 SeitenApproach To JaundiceNandita ChatterjeeNoch keine Bewertungen
- Assessing & Managing Urinary Tract DisordersDokument5 SeitenAssessing & Managing Urinary Tract DisordersAlyssa Nicole CajayonNoch keine Bewertungen
- Peptic Duodenal Ulcer History, Causes, Symptoms and TreatmentDokument106 SeitenPeptic Duodenal Ulcer History, Causes, Symptoms and TreatmentCanan YilmazNoch keine Bewertungen
- Lect - Peptic Ulcer - 211020 - 182113Dokument38 SeitenLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelNoch keine Bewertungen
- Peptic Ulcer of Stomach and DuodenumDokument59 SeitenPeptic Ulcer of Stomach and Duodenumchai rinNoch keine Bewertungen
- CHOLECYSTITISDokument6 SeitenCHOLECYSTITISAnar ChuluunNoch keine Bewertungen
- 2 Approach To Elevated LFTDokument59 Seiten2 Approach To Elevated LFTparik2321Noch keine Bewertungen
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryVon EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNoch keine Bewertungen
- Physiopathology SyllabusDokument1 SeitePhysiopathology SyllabusMohammad_Islam87Noch keine Bewertungen
- Lecture 17 DiabetesDokument51 SeitenLecture 17 DiabetesMohammad_Islam87Noch keine Bewertungen
- Lecture 20 CarcinogenesisDokument84 SeitenLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Abdominal HerniaeDokument66 SeitenAbdominal HerniaeMohammad_Islam87Noch keine Bewertungen
- The BreastDokument72 SeitenThe BreastMohammad_Islam87Noch keine Bewertungen
- Lecture 18 Upper Digestive DiseasesDokument63 SeitenLecture 18 Upper Digestive DiseasesMohammad_Islam87Noch keine Bewertungen
- The LymphomasDokument46 SeitenThe LymphomasMohammad_Islam87Noch keine Bewertungen
- Curst Um Abd EnglDokument10 SeitenCurst Um Abd EnglMohammad_Islam87Noch keine Bewertungen
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDokument18 SeitenMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87Noch keine Bewertungen
- Plastic SurgeryDokument11 SeitenPlastic SurgeryMohammad_Islam87Noch keine Bewertungen
- AnaemiaDokument83 SeitenAnaemiaMohammad_Islam87100% (2)
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDokument25 SeitenMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87Noch keine Bewertungen
- Pharmacology Lecture 19-5-2009, NSAIDSDokument19 SeitenPharmacology Lecture 19-5-2009, NSAIDSMohammad_Islam87Noch keine Bewertungen
- Liver Curs 2009Dokument215 SeitenLiver Curs 2009Mohammad_Islam87Noch keine Bewertungen
- Pharmacology Lecture 12-5-2009, OpiodsDokument18 SeitenPharmacology Lecture 12-5-2009, OpiodsMohammad_Islam87Noch keine Bewertungen
- Borcane TumorDokument14 SeitenBorcane TumorMohammad_Islam87Noch keine Bewertungen
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDokument29 SeitenMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87Noch keine Bewertungen
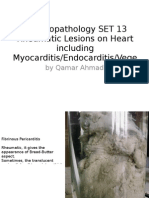
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDokument25 SeitenMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87Noch keine Bewertungen
- Pharmacology Lecture 5-5-2009Dokument15 SeitenPharmacology Lecture 5-5-2009Mohammad_Islam87Noch keine Bewertungen
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDokument19 SeitenMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87Noch keine Bewertungen
- Morphopathology Macroscopy (Romanian-Batch)Dokument187 SeitenMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Workshop 19Dokument3 SeitenWorkshop 19Mohammad_Islam87Noch keine Bewertungen
- Pharmacology Lecture Diuretic Agents (High Quality)Dokument15 SeitenPharmacology Lecture Diuretic Agents (High Quality)Mohammad_Islam87Noch keine Bewertungen
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokument7 SeitenBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Noch keine Bewertungen
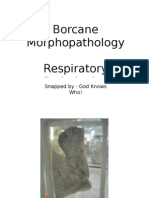
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokument11 SeitenBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87Noch keine Bewertungen
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDokument7 SeitenBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- ?#ry%oefr: - J4 @,8/ MryDokument15 Seiten?#ry%oefr: - J4 @,8/ MryMohammad_Islam87Noch keine Bewertungen
- Engl BUN - EditDokument167 SeitenEngl BUN - EditMohammad_Islam87Noch keine Bewertungen
- Workshop 20Dokument2 SeitenWorkshop 20Mohammad_Islam87Noch keine Bewertungen
- Conditions Presenting With Abdominal PainDokument69 SeitenConditions Presenting With Abdominal PainaimanNoch keine Bewertungen
- Patau Syndrome1Dokument5 SeitenPatau Syndrome1api-346355246Noch keine Bewertungen
- Report of Field Visit To National Centre For Disease ControlDokument12 SeitenReport of Field Visit To National Centre For Disease ControlVaishali JainarainNoch keine Bewertungen
- Nur 195 Case Study TemplateDokument14 SeitenNur 195 Case Study TemplateThyra Mae HisolerNoch keine Bewertungen
- Differential Diagnosis of Gastric CarcinomaDokument3 SeitenDifferential Diagnosis of Gastric CarcinomaNantini GopalNoch keine Bewertungen
- Urticaria and Angioedema - An Update On Classification and Pathogenesis PDFDokument14 SeitenUrticaria and Angioedema - An Update On Classification and Pathogenesis PDFancillaagraynNoch keine Bewertungen
- Herpes in PregnancyDokument3 SeitenHerpes in Pregnancyanon_841086875Noch keine Bewertungen
- How Can Blood Diseases Be IdentifiedDokument4 SeitenHow Can Blood Diseases Be Identifiedllatham0% (1)
- Manguiat, Ciara Loreal M. BSN 1-Y2-5 NCMA 111: Nursing Care PlanDokument3 SeitenManguiat, Ciara Loreal M. BSN 1-Y2-5 NCMA 111: Nursing Care PlanCiara ManguiatNoch keine Bewertungen
- How To Unlearn Your Pain - PositiveHealth PDFDokument5 SeitenHow To Unlearn Your Pain - PositiveHealth PDFEloy Vargas100% (1)
- Roberts, By: Cardiology 1993 E. Clinical Cardiology, 6th EditionDokument1 SeiteRoberts, By: Cardiology 1993 E. Clinical Cardiology, 6th EditionShiv GauravNoch keine Bewertungen
- DAFTAR PUSTAKA PebDokument2 SeitenDAFTAR PUSTAKA PebFatya WelinsaNoch keine Bewertungen
- Thesis On Type 2 Diabetes MellitusDokument6 SeitenThesis On Type 2 Diabetes Mellitusmoz1selajuk2100% (2)
- Depression Euphoria and Anger in The Emergency SettingDokument38 SeitenDepression Euphoria and Anger in The Emergency SettingpbsaintNoch keine Bewertungen
- Makalah Bahasa Inggris Unit 6Dokument10 SeitenMakalah Bahasa Inggris Unit 6Nadia NadNoch keine Bewertungen
- Mapeh QuizDokument6 SeitenMapeh Quizdalia antolinNoch keine Bewertungen
- CGHS Referral Procedure GuideDokument3 SeitenCGHS Referral Procedure GuideadhityaNoch keine Bewertungen
- Child Abuse and NeglectDokument23 SeitenChild Abuse and NeglectStephen StrangeNoch keine Bewertungen
- NEW CHECKLIST Endotracheal or Tracheal SuctioningDokument4 SeitenNEW CHECKLIST Endotracheal or Tracheal SuctioningDan Dan ManaoisNoch keine Bewertungen
- ARI CONTROL PROGRAMMEDokument13 SeitenARI CONTROL PROGRAMMEArun George50% (8)
- Hepatocellular Carcinoma (HCC)Dokument37 SeitenHepatocellular Carcinoma (HCC)Jeriz Marie GamboaNoch keine Bewertungen
- Penetrating Chest Trauma With Massive Hemothorax by A Small StoneDokument2 SeitenPenetrating Chest Trauma With Massive Hemothorax by A Small Stoneputri firda erlinaNoch keine Bewertungen
- A Mechanism-Based Approach To Clinical Reasoning of PainDokument9 SeitenA Mechanism-Based Approach To Clinical Reasoning of PainItai IzhakNoch keine Bewertungen
- Dermatology LexiconDokument5 SeitenDermatology LexiconMuhammad Luqman Nul HakimNoch keine Bewertungen
- RBSK New FormatDokument119 SeitenRBSK New Formatpvaibhav08100% (1)
- Levels of PreventionDokument53 SeitenLevels of PreventionsunielgowdaNoch keine Bewertungen
- Drug Card MotrinDokument2 SeitenDrug Card MotrinAdrianne BazoNoch keine Bewertungen
- TEMPLATE - Incident Report FormDokument3 SeitenTEMPLATE - Incident Report FormbesongNoch keine Bewertungen
- SOP Kids Club COVID 19 Measure For GO 2Dokument2 SeitenSOP Kids Club COVID 19 Measure For GO 2adjcdaughtNoch keine Bewertungen
- Clostridia and Bacillus Lecture NotesDokument37 SeitenClostridia and Bacillus Lecture NotesPrincewill SeiyefaNoch keine Bewertungen
- Levels of PreventionDokument12 SeitenLevels of PreventionRuth EkanemNoch keine Bewertungen