Das könnte Ihnen auch gefallen
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023Von EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Noch keine Bewertungen
- Acls MegacodeDokument8 SeitenAcls Megacodes33d_destinyNoch keine Bewertungen
- ACLS and PALS Certification Practice QuestionsDokument11 SeitenACLS and PALS Certification Practice Questionsdyah rahayu hutamiNoch keine Bewertungen
- Aha Acls Prep Packet 2020Dokument69 SeitenAha Acls Prep Packet 2020VP The Hacker100% (2)
- ACLS NotesDokument3 SeitenACLS Notessaxmanwrv0% (1)
- American Heart Association Acls Post Test AnswersDokument4 SeitenAmerican Heart Association Acls Post Test AnswersArun Jude Alphonse0% (9)
- ACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONDokument3 SeitenACLS PRETEST ANSWER KEY RHYTHM IDENTIFICATIONaditNoch keine Bewertungen
- 15 Item ACLS Drill With RationaleDokument12 Seiten15 Item ACLS Drill With RationaleLj Ferolino100% (1)
- ACLS Practice TestDokument5 SeitenACLS Practice Testprettynpink0867% (3)
- ACLS PrecourseAssessmentDokument19 SeitenACLS PrecourseAssessmentRaiedKhaled100% (1)
- ACLS (Advanced Cardiac Life Support) Algorithms & NotesDokument4 SeitenACLS (Advanced Cardiac Life Support) Algorithms & Notesiamlucil100% (4)
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDokument8 SeitenAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyNoch keine Bewertungen
- Cardiac Arrest Drugs & ProceduresDokument8 SeitenCardiac Arrest Drugs & ProceduresAstri Adel BudiarsoNoch keine Bewertungen
- ACLS Simulation ScenariosDokument14 SeitenACLS Simulation ScenariosVanessa HermioneNoch keine Bewertungen
- The Crash CartDokument39 SeitenThe Crash Cartpramod kumawat100% (1)
- CPR Class QuestionnaireDokument4 SeitenCPR Class QuestionnaireParikshit PekhaleNoch keine Bewertungen
- 2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes AlgorithmDokument1 Seite2010 Integrated Updated Circulation ACLS Acute Coronary Syndromes Algorithmms_lezahNoch keine Bewertungen
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDokument1 SeiteAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNoch keine Bewertungen
- TestDokument11 SeitenTestzenagit123456100% (1)
- AclsDokument85 SeitenAclsJulia CostaNoch keine Bewertungen
- ACLS QuizletDokument7 SeitenACLS Quizletek.9006001Noch keine Bewertungen
- ACLS Practice Test 1Dokument6 SeitenACLS Practice Test 1tarrynwortmann5319100% (3)
- Megacode Simulator 1Dokument10 SeitenMegacode Simulator 1srimatsimhasaneshwarNoch keine Bewertungen
- ACLS Full LectureDokument47 SeitenACLS Full LectureAdhydeva Purusanti100% (3)
- Emergency DrugsDokument26 SeitenEmergency DrugsSiergs Smith GervacioNoch keine Bewertungen
- ACLS Review Guide for Cardiac Arrest Scenarios and TreatmentDokument29 SeitenACLS Review Guide for Cardiac Arrest Scenarios and TreatmentJB Reyes100% (2)
- BLS and ACLS Case ScenariosDokument35 SeitenBLS and ACLS Case ScenariosrajNoch keine Bewertungen
- Introd To ECG Code Blue Champs March 2019Dokument52 SeitenIntrod To ECG Code Blue Champs March 2019james rukenya100% (1)
- ACLS DrugDokument7 SeitenACLS DrugPhongsatorn Thunin100% (1)
- ACLS Test PrintscreenedDokument13 SeitenACLS Test Printscreenedhellfireomega67% (9)
- Cals ReviewbjvjvjDokument14 SeitenCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- Nursing Responsibilities in Handling AntibioticsDokument4 SeitenNursing Responsibilities in Handling Antibioticsrichardmd20% (1)
- ACLS Written 2006 Precourse Self AssessmentDokument14 SeitenACLS Written 2006 Precourse Self AssessmentmonickamsNoch keine Bewertungen
- ACLS Precourse Test AnswersDokument60 SeitenACLS Precourse Test AnswersTip Piraya60% (5)
- ACLS Provider Manual Supplementary MaterialDokument86 SeitenACLS Provider Manual Supplementary MaterialEma0% (2)
- Soalan MCQ Acls Fit Set BDokument3 SeitenSoalan MCQ Acls Fit Set BAnonymous 89ilBIGhrmNoch keine Bewertungen
- ACLS Rhythms Practice Test 2020 Recognition Rhythm Strips (PDF)Dokument11 SeitenACLS Rhythms Practice Test 2020 Recognition Rhythm Strips (PDF)김민길100% (2)
- ACLS Exam - A&B VersionsDokument36 SeitenACLS Exam - A&B VersionsMohamed El-sayed100% (1)
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDokument8 SeitenACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
- ACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsDokument10 SeitenACLS Drugs: Primary Medications Used in Cardiac Arrest AlgorithmsChintami Octavia100% (1)
- ACLS FullMapsDokument68 SeitenACLS FullMapswong2689Noch keine Bewertungen
- ACLS Post Test (Copy) 낱말 카드 - QuizletDokument18 SeitenACLS Post Test (Copy) 낱말 카드 - Quizlet김민길Noch keine Bewertungen
- AclsDokument73 SeitenAclsKamel Hady50% (2)
- ACLS Algorithms SlideDokument26 SeitenACLS Algorithms SlidehrsoNoch keine Bewertungen
- BLS ALGORITHM As of February 2023Dokument2 SeitenBLS ALGORITHM As of February 2023Mark Jason Rodriguez, RNNoch keine Bewertungen
- ACLS ECG Rhythms & Pharmacology ReviewDokument24 SeitenACLS ECG Rhythms & Pharmacology Reviewkarenjlazarus86% (14)
- ACLS Provider Manual 2015 NotesDokument5 SeitenACLS Provider Manual 2015 Notescrystalshe93% (14)
- ACLS PrecourseAssessmentDokument19 SeitenACLS PrecourseAssessmentBrigitte Elaine81% (21)
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Cardio Pulmonary Resuscitation (CPR) and Automated External Defibrillation (AED) Training GuideVon EverandCardio Pulmonary Resuscitation (CPR) and Automated External Defibrillation (AED) Training GuideBewertung: 5 von 5 Sternen5/5 (1)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Advanced Cardiovascular Life Support (ACLS)Dokument27 SeitenAdvanced Cardiovascular Life Support (ACLS)Sara Ali100% (3)
- Managing Cardiac ArrestDokument12 SeitenManaging Cardiac ArrestpunctumlacrimaleNoch keine Bewertungen
- Guidelines Adult Advanced Life SupportDokument35 SeitenGuidelines Adult Advanced Life SupportindahNoch keine Bewertungen
- Advanced Cardiac Life Support: Valentina, MD, FIHADokument34 SeitenAdvanced Cardiac Life Support: Valentina, MD, FIHAfaradibaNoch keine Bewertungen
- CPR PDFDokument37 SeitenCPR PDFArdhi AgustjikNoch keine Bewertungen
- WHATs New in CPCRDokument4 SeitenWHATs New in CPCRJessicaHernandezNoch keine Bewertungen
- Gordon PDFDokument5 SeitenGordon PDFAthena SaturdayNoch keine Bewertungen
- Virginia Avenel HendersonDokument16 SeitenVirginia Avenel HendersonMark JosephNoch keine Bewertungen
- Question 1: What Is The PR Interval in This ECG?Dokument4 SeitenQuestion 1: What Is The PR Interval in This ECG?Mark JosephNoch keine Bewertungen
- Learning French EbookDokument36 SeitenLearning French EbookDonnette Davis100% (20)
- What Is CancerDokument13 SeitenWhat Is CancerMark JosephNoch keine Bewertungen
- Surgical and Radiation TherapyDokument22 SeitenSurgical and Radiation TherapyMark JosephNoch keine Bewertungen
- CT ShowDokument17 SeitenCT ShowMark JosephNoch keine Bewertungen
- Analysis and Evaluation of TheoriesDokument9 SeitenAnalysis and Evaluation of TheoriesMark JosephNoch keine Bewertungen
- Men in NursingDokument2 SeitenMen in NursingMark JosephNoch keine Bewertungen
- In Partial Fullfilment of The Course Requirements IN MSN 104: Clinical TeachingDokument6 SeitenIn Partial Fullfilment of The Course Requirements IN MSN 104: Clinical TeachingAnish VeettiyankalNoch keine Bewertungen
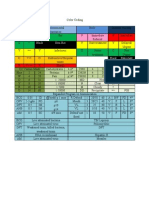
- Color Coding (CHN)Dokument1 SeiteColor Coding (CHN)Mark JosephNoch keine Bewertungen
- Diabetes Mellitus: Diagnostic ExamsDokument11 SeitenDiabetes Mellitus: Diagnostic ExamsMark JosephNoch keine Bewertungen
- Psycho PharmaDokument8 SeitenPsycho PharmaMark JosephNoch keine Bewertungen
- Patho InflammationDokument1 SeitePatho InflammationMark JosephNoch keine Bewertungen
- Diabetes Mellitus - Pathophysiological ParadigmDokument4 SeitenDiabetes Mellitus - Pathophysiological ParadigmMark JosephNoch keine Bewertungen
- RH Bill 2011Dokument31 SeitenRH Bill 2011Mark JosephNoch keine Bewertungen
- Fundamentals of NursingDokument4 SeitenFundamentals of NursingMark JosephNoch keine Bewertungen
- Types of FeedingDokument21 SeitenTypes of FeedingMark JosephNoch keine Bewertungen
- KuljeetDokument5 SeitenKuljeetSatyam TejiNoch keine Bewertungen
- WakoDokument2 SeitenWakoJimmy HarperNoch keine Bewertungen
- Clinical Exam RequirementDokument7 SeitenClinical Exam Requirementyb5fdt8cp7Noch keine Bewertungen
- Gordon's 11 Functional Health PatternDokument4 SeitenGordon's 11 Functional Health PatternVhince Norben PiscoNoch keine Bewertungen
- Raport StimulatorDokument88 SeitenRaport StimulatorEghet SilviuNoch keine Bewertungen
- Mitral Valve ProlapseDokument7 SeitenMitral Valve ProlapsehracakNoch keine Bewertungen
- Chest Pain DiagnosisDokument6 SeitenChest Pain DiagnosisJefri SoniNoch keine Bewertungen
- Puskesmas Cipadung Patient List December 2020Dokument65 SeitenPuskesmas Cipadung Patient List December 2020Aprilia PuspitasariNoch keine Bewertungen
- ACCSAP 10 Qs & As ReviewDokument470 SeitenACCSAP 10 Qs & As ReviewAdeel Lakhiar100% (8)
- Presentation 1Dokument12 SeitenPresentation 1Rizka FarahinNoch keine Bewertungen
- Britain: Nasty, British and ShortDokument3 SeitenBritain: Nasty, British and ShortLuana BarretoNoch keine Bewertungen
- Obesity - Kusimbisa: "Vanhu Vakawanda Munyika Varikufa Nokuda Kwekudya .... Kutopfuura Kufa Nenzara... " - BenjaminDokument8 SeitenObesity - Kusimbisa: "Vanhu Vakawanda Munyika Varikufa Nokuda Kwekudya .... Kutopfuura Kufa Nenzara... " - BenjaminMthabisi Tawanda NembawareNoch keine Bewertungen
- Pacemaker ThesisDokument4 SeitenPacemaker Thesissandraarvesethsaltlakecity100% (2)
- Nursing Care of Children with Cardiovascular DisordersDokument11 SeitenNursing Care of Children with Cardiovascular DisordersJœnríčk AzueloNoch keine Bewertungen
- Cardiac Sequential AnalysisDokument34 SeitenCardiac Sequential AnalysisMochamad Rizky HendiperdanaNoch keine Bewertungen
- Jambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)Dokument65 SeitenJambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)UPT PKM UJUNGBERUNG INDAHNoch keine Bewertungen
- Articulo - Theory and Desicion MakingDokument5 SeitenArticulo - Theory and Desicion MakingJaNe RNNoch keine Bewertungen
- Acs Guideline PDFDokument56 SeitenAcs Guideline PDFPrimasari HijriyahNoch keine Bewertungen
- 1-1-3 English CoreDokument11 Seiten1-1-3 English CoreRavneet KaurNoch keine Bewertungen
- Paralele Lijekova: Generičko Ime Djelovanje Tvorničko ImeDokument3 SeitenParalele Lijekova: Generičko Ime Djelovanje Tvorničko ImeStella GašparušNoch keine Bewertungen
- Estenosis Carotidea en Paciente Con Cardiopatía IsquémicaDokument57 SeitenEstenosis Carotidea en Paciente Con Cardiopatía IsquémicaSOLACI - Sociedad Latinoamericana de Cardiología IntervencionistaNoch keine Bewertungen
- Cardiac Arrest Upon Induction of General AnesthesiaDokument7 SeitenCardiac Arrest Upon Induction of General AnesthesiaIlona HiariejNoch keine Bewertungen
- L1 - SyncopeDokument5 SeitenL1 - SyncopeMuthukumaranNoch keine Bewertungen
- Jurnal Artikel Feby Nurlia 1907110032Dokument8 SeitenJurnal Artikel Feby Nurlia 1907110032Feby NurLiaNoch keine Bewertungen
- Rigel Uni Sim Lite DatasheetDokument5 SeitenRigel Uni Sim Lite Datasheetmailalexmd.vrn.ruNoch keine Bewertungen
- Physiology Lecture - Dr. Dominguez: Slow FastDokument3 SeitenPhysiology Lecture - Dr. Dominguez: Slow FastJayricDepalobosNoch keine Bewertungen
- NU 636 WK 2 DP 2 - Treatment of HyperlipidemiaDokument3 SeitenNU 636 WK 2 DP 2 - Treatment of HyperlipidemiaShayNoch keine Bewertungen
- ECG Guide: Understanding Waves, Intervals & Electrical EventsDokument164 SeitenECG Guide: Understanding Waves, Intervals & Electrical EventsMohsan RafiqNoch keine Bewertungen
- Errata updates for paspap 2nd Edition and Lang by Dr HameedDokument11 SeitenErrata updates for paspap 2nd Edition and Lang by Dr HameedUsama1987Noch keine Bewertungen
- Cap 6 Heart and Cardiovascular SystemDokument19 SeitenCap 6 Heart and Cardiovascular Systemgorexz goreNoch keine Bewertungen