Das könnte Ihnen auch gefallen
- Carcinoid Syndrome, A Simple Guide To The Condition, Treatment And Related DiseasesVon EverandCarcinoid Syndrome, A Simple Guide To The Condition, Treatment And Related DiseasesNoch keine Bewertungen
- Hypo Thyroid Is MDokument3 SeitenHypo Thyroid Is MjhNoch keine Bewertungen
- Thyroid HormoneDokument396 SeitenThyroid HormoneuiliftengNoch keine Bewertungen
- Paratiroid Dan KalsiumDokument80 SeitenParatiroid Dan KalsiumFebrina EvaNoch keine Bewertungen
- Clinical Review of Hereditary HaemochromatosisDokument6 SeitenClinical Review of Hereditary HaemochromatosisVijeyachandhar DorairajNoch keine Bewertungen
- Vitamins, minerals and trace elements essential guideDokument5 SeitenVitamins, minerals and trace elements essential guideCristhian LozanoNoch keine Bewertungen
- Reference Ranges For Blood TestsDokument38 SeitenReference Ranges For Blood TestscatalinNoch keine Bewertungen
- Electrolyte and Metabolic Panel GuideDokument24 SeitenElectrolyte and Metabolic Panel GuideDanish KamalNoch keine Bewertungen
- Liver Function Testing PDFDokument2 SeitenLiver Function Testing PDFRajesh KumarNoch keine Bewertungen
- Diabetic Neuropathy Treatment Case StudyDokument2 SeitenDiabetic Neuropathy Treatment Case Studyjonas1889Noch keine Bewertungen
- Metabolic Syndrome: Pennington Biomedical Research CenterDokument17 SeitenMetabolic Syndrome: Pennington Biomedical Research CenterJhay-arr HernandezNoch keine Bewertungen
- Hormone Therapy in The Postmenopausal Years - Considering Benefits and Risks in Clinical PracticDokument36 SeitenHormone Therapy in The Postmenopausal Years - Considering Benefits and Risks in Clinical PracticPaloma PeñaNoch keine Bewertungen
- Dr. Smijal PG Its Year Department of PeriodonticsDokument98 SeitenDr. Smijal PG Its Year Department of PeriodonticsMax FaxNoch keine Bewertungen
- Deficiency Disorders of Vitamins ExplainedDokument43 SeitenDeficiency Disorders of Vitamins ExplainedRENJINIRP100% (1)
- Kirk Man Beginners Guide WebDokument40 SeitenKirk Man Beginners Guide WebSophia Airall-ThomasNoch keine Bewertungen
- Calcium Metabolism PraveenDokument42 SeitenCalcium Metabolism PraveenDr PraveenNoch keine Bewertungen
- Mineral Metabolism and Abnormalities: Le Duong Hoang Huy M.D Email: Huyldh@pnt - Edu.vnDokument66 SeitenMineral Metabolism and Abnormalities: Le Duong Hoang Huy M.D Email: Huyldh@pnt - Edu.vnLam NgoNoch keine Bewertungen
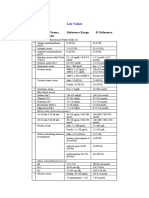
- Blood, Plasma, Serum Reference Range SI Reference: Lab ValuesDokument4 SeitenBlood, Plasma, Serum Reference Range SI Reference: Lab ValuesEvaG2012Noch keine Bewertungen
- Adrenal Gland OSCEDokument14 SeitenAdrenal Gland OSCEOmar AttaNoch keine Bewertungen
- Male Hypogonadism: EAU Guidelines OnDokument34 SeitenMale Hypogonadism: EAU Guidelines OnAyu sri WidianiNoch keine Bewertungen
- Diabetes Mellitus in The US:: PrevalenceDokument48 SeitenDiabetes Mellitus in The US:: PrevalenceokibreazyNoch keine Bewertungen
- AnemiaDokument41 SeitenAnemiaBang FadNoch keine Bewertungen
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionVon EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNoch keine Bewertungen
- Tumours of The Adrenal GlandDokument34 SeitenTumours of The Adrenal GlandSonam JoshiNoch keine Bewertungen
- Problem Based Learning Case Study Thyroid DisorderDokument30 SeitenProblem Based Learning Case Study Thyroid DisorderdrnawafNoch keine Bewertungen
- Microbiome impact on sex, thyroid, growth and parathyroid hormonesDokument13 SeitenMicrobiome impact on sex, thyroid, growth and parathyroid hormonesBrenda FolkNoch keine Bewertungen
- Check Unit 557 Jan-Feb Genetics v3 PDFDokument36 SeitenCheck Unit 557 Jan-Feb Genetics v3 PDFdragon66Noch keine Bewertungen
- Metabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseDokument40 SeitenMetabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseSatya FitriansyahNoch keine Bewertungen
- 14.human GeneticsDokument18 Seiten14.human GeneticsRenjith Moorikkaran MNoch keine Bewertungen
- Psychiatric effects of thyroid hormone disturbanceDokument9 SeitenPsychiatric effects of thyroid hormone disturbanceJosetta WhitneyNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyVon EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyBewertung: 1 von 5 Sternen1/5 (1)
- Atherosclerosis-Dyslipidaemia and Diabetes SlidesDokument83 SeitenAtherosclerosis-Dyslipidaemia and Diabetes SlidesECG17Noch keine Bewertungen
- Thyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistDokument30 SeitenThyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistNurul HikmaNoch keine Bewertungen
- Epilepsy: Causes of Seizures (Non-Epileptic)Dokument5 SeitenEpilepsy: Causes of Seizures (Non-Epileptic)humdingerNoch keine Bewertungen
- NSAIDs for Acute Gout AttacksDokument26 SeitenNSAIDs for Acute Gout AttacksReny Rony BersaudaraNoch keine Bewertungen
- Start Low and Go Slow 1-21-2014Dokument5 SeitenStart Low and Go Slow 1-21-2014Ed JonesNoch keine Bewertungen
- Sheehan SyndromeDokument6 SeitenSheehan SyndromeArvie TagnongNoch keine Bewertungen
- Constipation Risk Assessment ToolDokument2 SeitenConstipation Risk Assessment ToolAnggie Anggriyana100% (1)
- Oestrogen, Progesterone, AndrogensDokument58 SeitenOestrogen, Progesterone, AndrogensTandin SonamNoch keine Bewertungen
- Adrenal CrisisDokument27 SeitenAdrenal CrisissayednourNoch keine Bewertungen
- Guidelines & Protocols: Advisory CommitteeDokument9 SeitenGuidelines & Protocols: Advisory CommitteeeddcitoNoch keine Bewertungen
- Understanding Liver Tests and DiseasesDokument65 SeitenUnderstanding Liver Tests and DiseasesDokter MuhammadNoch keine Bewertungen
- G6PD Brochure 2017Dokument3 SeitenG6PD Brochure 2017Je Ann Catherine FeliasNoch keine Bewertungen
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Actions of Thyroid Hormone: Dr. Ayisha Qureshi Assistant Professor MBBS, MphilDokument41 SeitenActions of Thyroid Hormone: Dr. Ayisha Qureshi Assistant Professor MBBS, MphilJyoti ChadhaNoch keine Bewertungen
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDokument352 SeitenAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNoch keine Bewertungen
- HyperglycemiaDokument1 SeiteHyperglycemiaanon_262360776Noch keine Bewertungen
- Anemia Table283Dokument2 SeitenAnemia Table283Bridget ParkerNoch keine Bewertungen
- Steroid PathwaysDokument1 SeiteSteroid PathwaysCalvin ChiuNoch keine Bewertungen
- Liver Enzymes - ALT/ALT: DR - SarojaDokument15 SeitenLiver Enzymes - ALT/ALT: DR - SarojaSaroja VeereshNoch keine Bewertungen
- Metadichol: Rheumatoid Arthritis A Case StudyDokument4 SeitenMetadichol: Rheumatoid Arthritis A Case StudyDr P.R. RaghavanNoch keine Bewertungen
- Hyporeninemic HypoaldosteronismDokument12 SeitenHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNoch keine Bewertungen
- Parathyroid GlandsDokument4 SeitenParathyroid GlandsMary Grace Buscargas PolancosNoch keine Bewertungen
- ShockDokument63 SeitenShockshobharamkrishnaNoch keine Bewertungen
- Betty NeumanDokument15 SeitenBetty NeumanLiezel CauilanNoch keine Bewertungen
- Abdominal ExaminationDokument38 SeitenAbdominal ExaminationshobharamkrishnaNoch keine Bewertungen
- Abdominal ExaminationDokument38 SeitenAbdominal ExaminationshobharamkrishnaNoch keine Bewertungen
- Brain TumorDokument22 SeitenBrain TumorshobharamkrishnaNoch keine Bewertungen
- Ambulatory CareDokument7 SeitenAmbulatory CareshobharamkrishnaNoch keine Bewertungen
- Anatomy & Physiology of EyeDokument10 SeitenAnatomy & Physiology of EyeshobharamkrishnaNoch keine Bewertungen
- Anatomy & Physiology of the Nervous System - Parts, CNS, PNSDokument30 SeitenAnatomy & Physiology of the Nervous System - Parts, CNS, PNSshobharamkrishnaNoch keine Bewertungen
- Essential Guide to Dialysis TherapyDokument25 SeitenEssential Guide to Dialysis TherapyshobharamkrishnaNoch keine Bewertungen
- Electro Cardiogram & DysrythmiasDokument40 SeitenElectro Cardiogram & DysrythmiasshobharamkrishnaNoch keine Bewertungen
- HerniaDokument41 SeitenHerniashobharamkrishna67% (3)
- 101 - 36903 - Chapter 14 HairDokument17 Seiten101 - 36903 - Chapter 14 HairAaromal MaanasNoch keine Bewertungen
- Patient Ratio1:4Nurse:Patient Ratio1:6Intensive Care UnitNurse:Patient Ratio1:2Operating Room Nurse:Patient Ratio1:1Emergency RoomNurse:Patient Ratio1:3General Medical-SurgicalDokument53 SeitenPatient Ratio1:4Nurse:Patient Ratio1:6Intensive Care UnitNurse:Patient Ratio1:2Operating Room Nurse:Patient Ratio1:1Emergency RoomNurse:Patient Ratio1:3General Medical-SurgicalDarren FloresNoch keine Bewertungen
- Antisense Oligonucleotide Biotechnology, Applications and FutureDokument29 SeitenAntisense Oligonucleotide Biotechnology, Applications and FuturesurojitarpitaNoch keine Bewertungen
- Characteristics of Dyslexia PDFDokument3 SeitenCharacteristics of Dyslexia PDFDaniel Garzia Aizrag100% (2)
- NHS guidelines prevent refeeding syndromeDokument5 SeitenNHS guidelines prevent refeeding syndromePejman AhmadiNoch keine Bewertungen
- MSDS Sodium CarbonateDokument6 SeitenMSDS Sodium CarbonateEndang SupriyatnaNoch keine Bewertungen
- Exploring Nurses ' Experiences of Psychological Distress During Care of Patients With COVID-19: A Qualitative StudyDokument9 SeitenExploring Nurses ' Experiences of Psychological Distress During Care of Patients With COVID-19: A Qualitative StudyPinj BlueNoch keine Bewertungen
- Clinician S Guide To Neuropsychological AssessmentDokument538 SeitenClinician S Guide To Neuropsychological Assessmentmulix8880% (5)
- Suprarenal GlandDokument13 SeitenSuprarenal GlandAaa JjjjNoch keine Bewertungen
- Cell Parts and Their FunctionsDokument6 SeitenCell Parts and Their FunctionsJonathan MayoNoch keine Bewertungen
- EmbryologyDokument26 SeitenEmbryologyMeer BabanNoch keine Bewertungen
- Hypoxemia in ICU: Prepared by Hadi JazanDokument41 SeitenHypoxemia in ICU: Prepared by Hadi JazanHadi JazanNoch keine Bewertungen
- VSL TB Workplace Policy ProgramDokument3 SeitenVSL TB Workplace Policy ProgramAlexander John AlixNoch keine Bewertungen
- Discover the history of basil herb in this Wikipedia articleDokument8 SeitenDiscover the history of basil herb in this Wikipedia articleCinthia MarielaNoch keine Bewertungen
- Urinary Tract Infections in ChildrenDokument8 SeitenUrinary Tract Infections in ChildrenLorelie AsisNoch keine Bewertungen
- 8 Shaped WalkDokument1 Seite8 Shaped WalkAmy MyzaraNoch keine Bewertungen
- 25 OET Official Case Notes (Medicine)Dokument49 Seiten25 OET Official Case Notes (Medicine)Mesut KirazNoch keine Bewertungen
- Adrenergic Agonists Classification and EffectsDokument15 SeitenAdrenergic Agonists Classification and EffectsSeema YadavNoch keine Bewertungen
- Heart Failure (HF), Also Known As Congestive Heart Failure (CHF), Decompensatio Cordis (DC), and Congestive Cardiac Failure (CCF), IsDokument39 SeitenHeart Failure (HF), Also Known As Congestive Heart Failure (CHF), Decompensatio Cordis (DC), and Congestive Cardiac Failure (CCF), IsAbdurrahman AhzamiNoch keine Bewertungen
- Antenatal Power PointDokument135 SeitenAntenatal Power PointBULARON, Gerry Mar ANoch keine Bewertungen
- Sexual Health Education ToolkitDokument69 SeitenSexual Health Education ToolkitEndiNoch keine Bewertungen
- AnatomyDokument93 SeitenAnatomyHiba V.ANoch keine Bewertungen
- Paper For Enzyme ActivityDokument7 SeitenPaper For Enzyme ActivityFar hatNoch keine Bewertungen
- Description Device OLWA95005ADokument10 SeitenDescription Device OLWA95005AGabriela CenturiónNoch keine Bewertungen
- Ortho ExamDokument9 SeitenOrtho ExamPrince Rener Velasco Pera100% (2)
- 3767 11326 1 SMDokument9 Seiten3767 11326 1 SMGeztaNasafirHermawanNoch keine Bewertungen
- Preeclampsia and EclampsiaDokument24 SeitenPreeclampsia and EclampsiaFawzia Haznah Nurul ImaniNoch keine Bewertungen
- Journal of Health Global 2018Dokument344 SeitenJournal of Health Global 2018Rizki Agung PrasetyoNoch keine Bewertungen
- Core Course - Allied Health SciencesDokument31 SeitenCore Course - Allied Health SciencesMuhammad Sohail100% (1)