Das könnte Ihnen auch gefallen
- Feature StoriesDokument1 SeiteFeature StorieszerpthederpNoch keine Bewertungen
- Rheumatic Heart DiseaseDokument5 SeitenRheumatic Heart DiseasezerpthederpNoch keine Bewertungen
- CYSTOCLYSISDokument1 SeiteCYSTOCLYSISzerpthederpNoch keine Bewertungen
- Grand Cassade Study 1Dokument15 SeitenGrand Cassade Study 1zerpthederpNoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug Studyudntnid2knwme100% (4)
- Case Study of A Patient With Ischemic CardiomyopathyDokument33 SeitenCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- Requirements For Perpetual Succour Hospital PGNTDokument1 SeiteRequirements For Perpetual Succour Hospital PGNTzerpthederpNoch keine Bewertungen
- Drusadg Study For Paracetamol Omeprazole and Vitamin B ComplexDokument3 SeitenDrusadg Study For Paracetamol Omeprazole and Vitamin B ComplexzerpthederpNoch keine Bewertungen
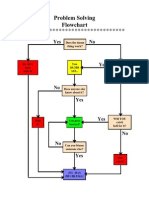
- Problem Solving Flowchart: Yes NoDokument1 SeiteProblem Solving Flowchart: Yes NozerpthederpNoch keine Bewertungen
- Psychiatric Nursing Bullets (Nle & Nclex)Dokument21 SeitenPsychiatric Nursing Bullets (Nle & Nclex)Richard Ines Valino100% (24)
- Laboratory ExamsDokument11 SeitenLaboratory ExamszerpthederpNoch keine Bewertungen
- Session 4: Main SymptomsDokument86 SeitenSession 4: Main SymptomszerpthederpNoch keine Bewertungen
- Compilation OF Case Studies: Perpetual Succour Hospital Gorordo Ave., Lahug, Cebu City Nursing Service DepartmentDokument1 SeiteCompilation OF Case Studies: Perpetual Succour Hospital Gorordo Ave., Lahug, Cebu City Nursing Service DepartmentzerpthederpNoch keine Bewertungen
- Grand Case Study 2Dokument2 SeitenGrand Case Study 2zerpthederpNoch keine Bewertungen
- Foetal CirculationDokument8 SeitenFoetal CirculationMujahid_Dean_8976Noch keine Bewertungen
- Community Needs AssessmentDokument13 SeitenCommunity Needs Assessmentzerpthederp0% (1)
- Bohol SUPREME STUDENT GOV'T Liquidation ReportDokument1 SeiteBohol SUPREME STUDENT GOV'T Liquidation ReportzerpthederpNoch keine Bewertungen
- UlcerDokument3 SeitenUlcerAjay SathyanNoch keine Bewertungen
- When in Rome PDFDokument120 SeitenWhen in Rome PDFzerpthederpNoch keine Bewertungen
- CokeDokument3 SeitenCokezerpthederpNoch keine Bewertungen
- UBCN Nursing Staff Event SponsorshipDokument2 SeitenUBCN Nursing Staff Event SponsorshipzerpthederpNoch keine Bewertungen
- Welcome AddressDokument1 SeiteWelcome AddresszerpthederpNoch keine Bewertungen
- NMAT ID Form-1111302389Dokument1 SeiteNMAT ID Form-1111302389zerpthederpNoch keine Bewertungen
- Identifying Our Own ProblemsDokument8 SeitenIdentifying Our Own ProblemszerpthederpNoch keine Bewertungen
- 12 Literary Compositions That Have Influenced The WorldDokument3 Seiten12 Literary Compositions That Have Influenced The Worldzerpthederp100% (6)
- CIM Application Form 1Dokument1 SeiteCIM Application Form 1Kara AguilarNoch keine Bewertungen
- Dengue Fever Case StudyDokument24 SeitenDengue Fever Case Studymaemaeyee95% (22)
- Session 4: Main SymptomsDokument86 SeitenSession 4: Main SymptomszerpthederpNoch keine Bewertungen
- UBCN Nursing Event SponsorshipDokument3 SeitenUBCN Nursing Event SponsorshipzerpthederpNoch keine Bewertungen
- TOPICDokument1 SeiteTOPICzerpthederpNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Rha GGBS 27 4Dokument12 SeitenRha GGBS 27 4KhaDeja MawraNoch keine Bewertungen
- 3 - 6consctructing Probability Distributions CG A - 4 - 6 Lesson 2Dokument24 Seiten3 - 6consctructing Probability Distributions CG A - 4 - 6 Lesson 2CHARLYN JOY SUMALINOGNoch keine Bewertungen
- Laser Engrave Co2 System BJ-1390Dokument5 SeitenLaser Engrave Co2 System BJ-1390Sasa TodorovicNoch keine Bewertungen
- Absolute Value - WikipediaDokument10 SeitenAbsolute Value - WikipediaVenu GopalNoch keine Bewertungen
- Generate Ideas with TechniquesDokument19 SeitenGenerate Ideas with TechniquesketulNoch keine Bewertungen
- A Laboratory Experiment in Crystals and Crystal Model Building ObjectivesDokument7 SeitenA Laboratory Experiment in Crystals and Crystal Model Building ObjectivesrajaaNoch keine Bewertungen
- PEB Requirment by ClientDokument4 SeitenPEB Requirment by ClientViraj ModiNoch keine Bewertungen
- Brochure HorticultureDokument46 SeitenBrochure HorticulturezulfiqaralimalikNoch keine Bewertungen
- PoiconverterDokument2 SeitenPoiconvertertaco6541Noch keine Bewertungen
- Inclusive E-Service or Risk of Digital Divide The Case of National ICT Policy 2018 of BangladeshDokument11 SeitenInclusive E-Service or Risk of Digital Divide The Case of National ICT Policy 2018 of BangladeshInternational Journal of Innovative Science and Research Technology100% (1)
- Hematology NotesDokument3 SeitenHematology NotesFarisa Jane BanggoNoch keine Bewertungen
- MATH6113 - PPT5 - W5 - R0 - Applications of IntegralsDokument58 SeitenMATH6113 - PPT5 - W5 - R0 - Applications of IntegralsYudho KusumoNoch keine Bewertungen
- Hong Kong A-Level Chemistry Book 3ADokument69 SeitenHong Kong A-Level Chemistry Book 3AMARENG BERNABENoch keine Bewertungen
- Sustaining The Metropolis: LRT and Streetcars For Super Cities, Presented by The Transportation Research Board of The National Academies (Circular E-C177)Dokument408 SeitenSustaining The Metropolis: LRT and Streetcars For Super Cities, Presented by The Transportation Research Board of The National Academies (Circular E-C177)Randall WestNoch keine Bewertungen
- Physics MCQ Solid State PhysicsDokument15 SeitenPhysics MCQ Solid State PhysicsRams Chander88% (25)
- Educating The PosthumanDokument50 SeitenEducating The PosthumanCatherine BrugelNoch keine Bewertungen
- DelhiDokument40 SeitenDelhiRahul DharNoch keine Bewertungen
- VANSINA, Jan. Art History in AfricaDokument250 SeitenVANSINA, Jan. Art History in AfricaRaphaelTim100% (1)
- Literature Review Marketing StrategyDokument4 SeitenLiterature Review Marketing Strategyc5td1cmc100% (1)
- Questions 32 - 34: Sunny English MqaDokument9 SeitenQuestions 32 - 34: Sunny English MqaHạnh NguyễnNoch keine Bewertungen
- Tos IcuDokument1 SeiteTos IcuMary Cris RombaoaNoch keine Bewertungen
- Predictive Analytics: QM901.1x Prof U Dinesh Kumar, IIMBDokument36 SeitenPredictive Analytics: QM901.1x Prof U Dinesh Kumar, IIMBVenkata Nelluri PmpNoch keine Bewertungen
- ZJJ 3Dokument23 SeitenZJJ 3jananiwimukthiNoch keine Bewertungen
- FD-BF-001 Foxboro FieldDevices 010715 LowRes PDFDokument24 SeitenFD-BF-001 Foxboro FieldDevices 010715 LowRes PDFThiago FernandesNoch keine Bewertungen
- Argenti, P. Corporate Communication. Cap. 8-9Dokument28 SeitenArgenti, P. Corporate Communication. Cap. 8-9juan100% (1)
- Metal Oxides Semiconductor CeramicsDokument14 SeitenMetal Oxides Semiconductor Ceramicsumarasad1100% (1)
- My ResumeDokument4 SeitenMy Resumeapi-216740002Noch keine Bewertungen
- About Topsøe - and What We DoDokument20 SeitenAbout Topsøe - and What We DoAbhishek ChaudharyNoch keine Bewertungen
- Adventures in PioneeringDokument202 SeitenAdventures in PioneeringShawn GuttmanNoch keine Bewertungen
- Chime Primary School Brochure TemplateDokument1 SeiteChime Primary School Brochure TemplateNita HanifahNoch keine Bewertungen