Das könnte Ihnen auch gefallen
- Drug-Receptor Interactions AND Pharmacodynamics: Ramla KashifDokument36 SeitenDrug-Receptor Interactions AND Pharmacodynamics: Ramla KashifRamla KashifNoch keine Bewertungen
- Molecular Drug Binding PrinciplesDokument100 SeitenMolecular Drug Binding PrinciplesagnespaungNoch keine Bewertungen
- Malnutrition among under-5 children and health service delivery by Village Health TeamsDokument23 SeitenMalnutrition among under-5 children and health service delivery by Village Health TeamsBheru Lal100% (1)
- 2nd Lecture On Action Potential by Dr. Roomi.Dokument14 Seiten2nd Lecture On Action Potential by Dr. Roomi.Mudassar Roomi100% (1)
- LipidsDokument13 SeitenLipidsalianaNoch keine Bewertungen
- Metabolism of Carbohydrates, Lipids, Amino Acids and its Regulation Test QuestionsDokument209 SeitenMetabolism of Carbohydrates, Lipids, Amino Acids and its Regulation Test Questionsninas1112Noch keine Bewertungen
- Mad Chum-I Biosynthesis A Catabolism of CotecholaminesDokument4 SeitenMad Chum-I Biosynthesis A Catabolism of CotecholaminesLalit SharmaNoch keine Bewertungen
- Digestion & Absorption of CarbohydratesDokument14 SeitenDigestion & Absorption of CarbohydratesKuzhandai VeluNoch keine Bewertungen
- Routes of Drug EliminationDokument17 SeitenRoutes of Drug EliminationdahiphalehNoch keine Bewertungen
- Pharmacology:MIT:Anti Arrythmics 4Dokument17 SeitenPharmacology:MIT:Anti Arrythmics 4Louis FortunatoNoch keine Bewertungen
- Nuclear Receptors 2006Dokument31 SeitenNuclear Receptors 2006lsintaningtyasNoch keine Bewertungen
- Amino Acid Catabolism Between OrgansDokument44 SeitenAmino Acid Catabolism Between OrgansFarhati MardhiyahNoch keine Bewertungen
- Carbohydrate MetabolismDokument57 SeitenCarbohydrate MetabolismYulliza Kurniawaty L100% (1)
- Classification and Nomenclature of EnzymesDokument12 SeitenClassification and Nomenclature of EnzymesmcgilicuttyNoch keine Bewertungen
- Class Notes of Amino Acid MetabolismDokument49 SeitenClass Notes of Amino Acid MetabolismShivanand Mali100% (1)
- Urine Formation: Reabsorption and Secretion, and Water ConservationDokument5 SeitenUrine Formation: Reabsorption and Secretion, and Water ConservationAshraf Moby100% (1)
- Lipoprotein MetabolismDokument60 SeitenLipoprotein MetabolismI MADE MIARTA YASANoch keine Bewertungen
- Kidney Nephron Structure and FunctionDokument4 SeitenKidney Nephron Structure and Functionxanxan4321Noch keine Bewertungen
- Enzyme Inducers and Inhibitors TransDokument6 SeitenEnzyme Inducers and Inhibitors TransLeonallee MayorNoch keine Bewertungen
- Glomerular Function TestsDokument26 SeitenGlomerular Function TestsAvi Verma100% (1)
- 15G Protein-Coupled ReceptorDokument15 Seiten15G Protein-Coupled ReceptorZiedTrikiNoch keine Bewertungen
- Cell Junctions by DR RoomiDokument15 SeitenCell Junctions by DR RoomiMudassar Roomi100% (1)
- GPCR 160211124029Dokument83 SeitenGPCR 160211124029JuhiJahan AmanullahNoch keine Bewertungen
- Neuron Structure and Function: Active Lecture Question Slides Prepared by Dr. Alan F. Smith, Mercer UniversityDokument105 SeitenNeuron Structure and Function: Active Lecture Question Slides Prepared by Dr. Alan F. Smith, Mercer UniversityDenden Gamboa100% (1)
- Urea CycleDokument22 SeitenUrea CycleDawlat SalamaNoch keine Bewertungen
- NPN Compounds: Urea, Creatinine, Uric Acid & AmmoniaDokument37 SeitenNPN Compounds: Urea, Creatinine, Uric Acid & AmmoniaMustafa KhandgawiNoch keine Bewertungen
- Neuromuscular Junction by Dr. RoomiDokument20 SeitenNeuromuscular Junction by Dr. RoomiMudassar Roomi100% (1)
- Carbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiDokument6 SeitenCarbohydrate Metabolism: Blood Haemoglobin and Respiration: - Archit SaraogiChictoran RukmaniNoch keine Bewertungen
- Pharmacokinetics lecture notes on absorption, distribution, metabolism, and excretion (ADMEDokument4 SeitenPharmacokinetics lecture notes on absorption, distribution, metabolism, and excretion (ADMEfaithsheepNoch keine Bewertungen
- Enzyme Kinetics NotesDokument2 SeitenEnzyme Kinetics NotesMarc Imhotep Cray, M.D.Noch keine Bewertungen
- Histology of Synapse and Neuroglia by Dr. RoomiDokument18 SeitenHistology of Synapse and Neuroglia by Dr. RoomiMudassar Roomi100% (1)
- Acetylcholine Stimulates Muscle Contraction in Guinea Pig Ileum and Atropine Diminishes The Extent of ContractionDokument2 SeitenAcetylcholine Stimulates Muscle Contraction in Guinea Pig Ileum and Atropine Diminishes The Extent of Contractionleh.mo931580% (5)
- Antiplatelet and Thrombolytic DrugsDokument48 SeitenAntiplatelet and Thrombolytic DrugsNofa PuspitaNoch keine Bewertungen
- Ch5 Cell SignallingDokument50 SeitenCh5 Cell SignallingShatha KhzaimiahNoch keine Bewertungen
- Cell Signaling in Space and Time:: Where Proteins Come Together and When They're ApartDokument20 SeitenCell Signaling in Space and Time:: Where Proteins Come Together and When They're ApartHumbertoNoch keine Bewertungen
- Pharm QuestionsDokument5 SeitenPharm Questionsvaroon525Noch keine Bewertungen
- Tubular ReabsorptionDokument42 SeitenTubular Reabsorptionmina mounirNoch keine Bewertungen
- G-Protein Coupled ReceptorsDokument8 SeitenG-Protein Coupled ReceptorsHyunji KimNoch keine Bewertungen
- Physiology of ANS Lecture 1 by Dr. Mudassar Ali RoomiDokument19 SeitenPhysiology of ANS Lecture 1 by Dr. Mudassar Ali RoomiMudassar RoomiNoch keine Bewertungen
- Mechanism of Buffering SystemDokument8 SeitenMechanism of Buffering SystemRezaul Karim TutulNoch keine Bewertungen
- Carboxy PeptidaseDokument17 SeitenCarboxy PeptidaseReyadevi G100% (1)
- Digestive System NotesDokument10 SeitenDigestive System NotesArchanna VyassNoch keine Bewertungen
- Drug MetabolismDokument78 SeitenDrug Metabolismjuz gonzagaNoch keine Bewertungen
- Cagayan State University College of Medicine and Surgery SY: 2009-2010Dokument41 SeitenCagayan State University College of Medicine and Surgery SY: 2009-2010ahmad usmanNoch keine Bewertungen
- Histology of Pancreas by Dr. RoomiDokument20 SeitenHistology of Pancreas by Dr. RoomiMudassar Roomi100% (1)
- Biochemistry Lecture 2 Cell and OrganellesDokument16 SeitenBiochemistry Lecture 2 Cell and OrganellesProfessor Rakesh Sharma Biochemistry LecturesNoch keine Bewertungen
- Understanding Metabolism of CarbohydratesDokument48 SeitenUnderstanding Metabolism of CarbohydratesAbdullah TheNoch keine Bewertungen
- Drug Heart Failure MDokument24 SeitenDrug Heart Failure MAthari KhanNoch keine Bewertungen
- The Adrenal GlandDokument41 SeitenThe Adrenal GlandRujha Haniena Ahmad RidzuanNoch keine Bewertungen
- Biochemistry One LinersDokument11 SeitenBiochemistry One Linerssandeep MahapatraNoch keine Bewertungen
- Disorders of Purine and Pyrimidine MetabolismDokument17 SeitenDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNoch keine Bewertungen
- Clinical EnzymologyDokument25 SeitenClinical Enzymologyaminata6Noch keine Bewertungen
- Enzymes: Protein Catalysts That Increase The Rate of Reactions Without Being Changed in The Overall ProcessDokument49 SeitenEnzymes: Protein Catalysts That Increase The Rate of Reactions Without Being Changed in The Overall ProcessGhafoor AzamNoch keine Bewertungen
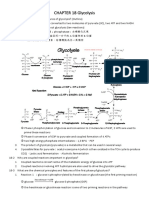
- CHAPTER 18 GlycolysisDokument10 SeitenCHAPTER 18 Glycolysis楊畯凱Noch keine Bewertungen
- Thyroid Gland BasicsDokument25 SeitenThyroid Gland BasicsSreekar DevarakondaNoch keine Bewertungen
- Pharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedDokument47 SeitenPharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedAshaNoch keine Bewertungen
- Medicinal Chemistry of Beta-Lactam AntibioticsDokument13 SeitenMedicinal Chemistry of Beta-Lactam AntibioticsJosiah O OmobaNoch keine Bewertungen
- CH 11 PPT Cell Communication 1Dokument77 SeitenCH 11 PPT Cell Communication 1api-270681964Noch keine Bewertungen
- Receptors IntroductionDokument53 SeitenReceptors IntroductionSunilNoch keine Bewertungen
- Mechanism of Drug ActionDokument24 SeitenMechanism of Drug ActionBandita Datta100% (1)
- Mycotoxins and Bacterial Toxins: Types, Characteristics and EffectsDokument103 SeitenMycotoxins and Bacterial Toxins: Types, Characteristics and EffectsSunil100% (1)
- Household Hazards To PetsDokument16 SeitenHousehold Hazards To PetsSunilNoch keine Bewertungen
- Drugs in ReptilesDokument71 SeitenDrugs in ReptilesSunil100% (1)
- Drugs in Behavioural Disorders of PetsDokument5 SeitenDrugs in Behavioural Disorders of PetsSunilNoch keine Bewertungen
- Carbon Monoxide PoisoningDokument22 SeitenCarbon Monoxide PoisoningSunilNoch keine Bewertungen
- VCI MSVE 2008 RegulationsDokument136 SeitenVCI MSVE 2008 RegulationsSunil50% (2)
- FLUORINE TOXICITY AND FLUOROSISDokument55 SeitenFLUORINE TOXICITY AND FLUOROSISSunilNoch keine Bewertungen
- ENDOCRINE PHARMACOLOGY: THYROID AND PANCREATIC HORMONESDokument16 SeitenENDOCRINE PHARMACOLOGY: THYROID AND PANCREATIC HORMONESSunilNoch keine Bewertungen
- Veterinary Pharmacology and Toxicology MCQsDokument10 SeitenVeterinary Pharmacology and Toxicology MCQsSunilNoch keine Bewertungen
- Classification of AmphibiansDokument22 SeitenClassification of AmphibiansSunilNoch keine Bewertungen
- Toxicological Investigation and Its Significance in Animal Health DiagnosisDokument8 SeitenToxicological Investigation and Its Significance in Animal Health DiagnosisSunilNoch keine Bewertungen
- Classification and Dosage of Antimicrobial Agents in Veterinary MedicineDokument24 SeitenClassification and Dosage of Antimicrobial Agents in Veterinary MedicineSunil0% (1)
- Nsaids and Other Antinflammatory Agents in Veterinary PracticeDokument44 SeitenNsaids and Other Antinflammatory Agents in Veterinary PracticeSunil100% (2)
- Antiseptics and Disinfectants For Veterinary ClinicsDokument3 SeitenAntiseptics and Disinfectants For Veterinary ClinicsSunil100% (5)
- Drugs Acting On Respiratory System of AnimalsDokument8 SeitenDrugs Acting On Respiratory System of AnimalsSunil100% (4)
- Drugs Acting On Genitourinary System of AnimalsDokument44 SeitenDrugs Acting On Genitourinary System of AnimalsSunilNoch keine Bewertungen
- Drugs Acting On Digestive System of AnimalsDokument11 SeitenDrugs Acting On Digestive System of AnimalsSunil100% (3)
- Drugs Acting On Haematopoietic System of AnimalsDokument28 SeitenDrugs Acting On Haematopoietic System of AnimalsSunil100% (1)
- Behavioural Modifying Drugs in PetsDokument33 SeitenBehavioural Modifying Drugs in PetsSunilNoch keine Bewertungen
- Mercury Lead Arsenic Cadmium ToxicityDokument171 SeitenMercury Lead Arsenic Cadmium ToxicitySunilNoch keine Bewertungen
- LATHYRISM AND PHOTOSENSiTIZATIONDokument33 SeitenLATHYRISM AND PHOTOSENSiTIZATIONSunilNoch keine Bewertungen
- GENERAL LINE of Treatment UREA AMMONIA SALT - poISONINGDokument49 SeitenGENERAL LINE of Treatment UREA AMMONIA SALT - poISONINGSunil0% (1)
- Environmental PollutantsDokument32 SeitenEnvironmental PollutantsSunilNoch keine Bewertungen
- Toxicokinetics DynamicsDokument76 SeitenToxicokinetics DynamicsSunil100% (1)
- Site of Action of Drugs Acting On Cholinergic Neurohumoral Transmission PDFDokument1 SeiteSite of Action of Drugs Acting On Cholinergic Neurohumoral Transmission PDFSunilNoch keine Bewertungen
- Site of Action of Drugs Acting On Adrenergic Neurohumoral Transmission PDFDokument1 SeiteSite of Action of Drugs Acting On Adrenergic Neurohumoral Transmission PDFSunilNoch keine Bewertungen
- ZOOTOXINSDokument72 SeitenZOOTOXINSSunil83% (6)
- Fluorosis Phosphorous ToxicityDokument55 SeitenFluorosis Phosphorous ToxicitySunilNoch keine Bewertungen
- Mycotoxins and Bacterial Toxins: Types, Characteristics and EffectsDokument103 SeitenMycotoxins and Bacterial Toxins: Types, Characteristics and EffectsSunil100% (1)
- Epilepsy and Anticonvulsant DrugsDokument28 SeitenEpilepsy and Anticonvulsant DrugsSunilNoch keine Bewertungen
- J Exp Med 1991 Linsley 721 30Dokument10 SeitenJ Exp Med 1991 Linsley 721 30Fernanda RibeiroNoch keine Bewertungen
- Concurrent Strength and Endurance Training: From Molecules To ManDokument7 SeitenConcurrent Strength and Endurance Training: From Molecules To Manjtin_scribdNoch keine Bewertungen
- Microsyllabus BSC 301Dokument9 SeitenMicrosyllabus BSC 301Anwita JhaNoch keine Bewertungen
- PD22 Hap1 L03Dokument33 SeitenPD22 Hap1 L03Ka Yan LAUNoch keine Bewertungen
- Alexander Et Al-2011-British Journal of PharmacologyDokument326 SeitenAlexander Et Al-2011-British Journal of PharmacologyDNav14Noch keine Bewertungen
- Cell Signaling Webquest: Part 1: Dropping SignalsDokument3 SeitenCell Signaling Webquest: Part 1: Dropping Signalsa60ONoch keine Bewertungen
- DRUG RECEPTORS and PHARMACODYNAMICSDokument105 SeitenDRUG RECEPTORS and PHARMACODYNAMICSaben101781Noch keine Bewertungen
- Host ModulationDokument101 SeitenHost ModulationVikrant SainiaNoch keine Bewertungen
- Introduction To Neurotransmitters: BY: Mudasir Maqbool Mohmad Amin DarDokument24 SeitenIntroduction To Neurotransmitters: BY: Mudasir Maqbool Mohmad Amin DarKAMYA SRIDHARAN 20214044100% (1)
- Opioid Receptors: J Mcdonald PHD DG Lambert PHD FrcaDokument6 SeitenOpioid Receptors: J Mcdonald PHD DG Lambert PHD Frcagigidurul1111Noch keine Bewertungen
- #Cartography 2 - Centers - RaDokument53 Seiten#Cartography 2 - Centers - RaDorabella100% (1)
- Formula Mass and the Mole Concept ExplainedDokument14 SeitenFormula Mass and the Mole Concept ExplainedJonalyn VitalicioNoch keine Bewertungen
- Metabolic SD in Clinical PracticeDokument268 SeitenMetabolic SD in Clinical PracticePetzyMarianNoch keine Bewertungen
- Genetics of Human ObesityDokument14 SeitenGenetics of Human Obesitymuralidhar_mettaNoch keine Bewertungen
- NB000573Dokument513 SeitenNB000573Avrupa Birliği Enstitüsü100% (2)
- EmbryologyDokument215 SeitenEmbryologyMunewer AbdellaNoch keine Bewertungen
- Structure Activity Relationships of Phenylalkylamines As Agonist Ligands For 5 HT2ADokument11 SeitenStructure Activity Relationships of Phenylalkylamines As Agonist Ligands For 5 HT2ALUCAS OYANEDERNoch keine Bewertungen
- Plan Diagram of The Tissues 2Dokument32 SeitenPlan Diagram of The Tissues 2BonnyNoch keine Bewertungen
- NLRP3 InflammasomeDokument11 SeitenNLRP3 InflammasomeUmmuNoch keine Bewertungen
- Build A Paper Model of A G Protein-Coupled Receptor (GPCR) : Preparation Alpha Helices and Polymer ChainDokument3 SeitenBuild A Paper Model of A G Protein-Coupled Receptor (GPCR) : Preparation Alpha Helices and Polymer Chainnewt03abNoch keine Bewertungen
- AP Biology Name Guided Reading Chapter 39: Weston BaumannDokument6 SeitenAP Biology Name Guided Reading Chapter 39: Weston BaumannWeston Baumann50% (2)
- Foundations in Biology Exam 2 NotesDokument2 SeitenFoundations in Biology Exam 2 NotesMatt ParkNoch keine Bewertungen
- TOPIC 4.1-4.4 - Cell Communication, Cell Signaling SMV Student Learning Guide, 2020Dokument6 SeitenTOPIC 4.1-4.4 - Cell Communication, Cell Signaling SMV Student Learning Guide, 2020L ChanNoch keine Bewertungen
- Nino Gachechiladze ImunitetiDokument268 SeitenNino Gachechiladze ImunitetiSaba GabadzeNoch keine Bewertungen
- Bio BookDokument1.578 SeitenBio BookAmeen Anwar100% (3)
- Full Test Bank For Understanding Pathophysiology 6Th Edition by Huether PDF Docx Full Chapter ChapterDokument36 SeitenFull Test Bank For Understanding Pathophysiology 6Th Edition by Huether PDF Docx Full Chapter Chapterexequycheluract6oi100% (8)
- 1841846791Dokument600 Seiten1841846791Mohammed Hussein100% (1)
- Molecules: Anti-Depressive Effectiveness of Baicalin in Vitro and in VivoDokument13 SeitenMolecules: Anti-Depressive Effectiveness of Baicalin in Vitro and in VivoMylena SilvaNoch keine Bewertungen
- Targeting The IL-17 Pathway in Inflammatory Disease: Pierre MiossecDokument1 SeiteTargeting The IL-17 Pathway in Inflammatory Disease: Pierre Miossecanirbanmanna88320100% (1)
- Mendel Et Al 2003Dokument12 SeitenMendel Et Al 2003Selliana Maretha Wijaya KusumaNoch keine Bewertungen