Das könnte Ihnen auch gefallen
- BRAIN Tumors PDFDokument44 SeitenBRAIN Tumors PDFHalima Assi100% (1)
- Brain TumorsDokument72 SeitenBrain Tumorsmo_mibNoch keine Bewertungen
- Glioma - Chinh SuaDokument176 SeitenGlioma - Chinh SuaHikari AoiNoch keine Bewertungen
- Brain TumorsDokument43 SeitenBrain TumorsDanaNoch keine Bewertungen
- Brain Tumours Imaging-1Dokument20 SeitenBrain Tumours Imaging-1HusseinNoch keine Bewertungen
- Brain TumorsDokument78 SeitenBrain Tumorsnarswiponshistoryan100% (3)
- Neuropathology: FK UisuDokument28 SeitenNeuropathology: FK UisuAnggi WahyuNoch keine Bewertungen
- 03 TumoursDokument50 Seiten03 TumoursMalinda KarunaratneNoch keine Bewertungen
- CNS TumorDokument32 SeitenCNS TumorBbem ooNoch keine Bewertungen
- Brain TumorsDokument11 SeitenBrain TumorsAmmar Bin KhalilNoch keine Bewertungen
- Spinaltumors Copy 160925185617Dokument122 SeitenSpinaltumors Copy 160925185617Irving H Torres LopezNoch keine Bewertungen
- Intramedullary Spinal Cord Tumors: Clinical PresentationDokument15 SeitenIntramedullary Spinal Cord Tumors: Clinical Presentationmetasoniko81Noch keine Bewertungen
- CNS Pathology Course: - Recommended TextbookDokument39 SeitenCNS Pathology Course: - Recommended TextbookchinnnababuNoch keine Bewertungen
- CNS Tumors: Adult Tumors Tend To Be Supratentorial (70%) Pediatric Tumors Tend To Be Infratentorial (70%)Dokument8 SeitenCNS Tumors: Adult Tumors Tend To Be Supratentorial (70%) Pediatric Tumors Tend To Be Infratentorial (70%)Jessica Febrina WuisanNoch keine Bewertungen
- SDL 8 Intracranial Space Occupying LesionDokument5 SeitenSDL 8 Intracranial Space Occupying LesionJonathan YeohNoch keine Bewertungen
- Cerebral Metastasis: Syed Maroof AliDokument28 SeitenCerebral Metastasis: Syed Maroof AliMaroofAliNoch keine Bewertungen
- Ventricular LesionsDokument76 SeitenVentricular LesionsIslam AghouryNoch keine Bewertungen
- Agarwal 2016Dokument51 SeitenAgarwal 2016Daniel Alfredo Tenorio GonzálezNoch keine Bewertungen
- Tumors of CNS: MBBS, FCPS, M.Phil. Histopathology Department of PathologyDokument23 SeitenTumors of CNS: MBBS, FCPS, M.Phil. Histopathology Department of PathologyOga bogaNoch keine Bewertungen
- B.2. 0Dokument7 SeitenB.2. 0Bahna LucianNoch keine Bewertungen
- MedulloblastomaDokument6 SeitenMedulloblastomaMohammadAwitNoch keine Bewertungen
- Sol IntracranialDokument76 SeitenSol IntracranialPanduRespatiNoch keine Bewertungen
- Foaie de CoptDokument105 SeitenFoaie de CoptVlad Octavian BolocanNoch keine Bewertungen
- BRAIN NEOPLASMS ON YOUR DINNER TABLE Dr. A.OdhiamboDokument74 SeitenBRAIN NEOPLASMS ON YOUR DINNER TABLE Dr. A.OdhiamboMalueth AnguiNoch keine Bewertungen
- Embryonal TumoursDokument11 SeitenEmbryonal TumoursAhmad YasserNoch keine Bewertungen
- NEUROPATHOLOGYDokument28 SeitenNEUROPATHOLOGYPratama SutardiNoch keine Bewertungen
- Phyllodes TumorDokument20 SeitenPhyllodes TumorManuela KarinaaNoch keine Bewertungen
- Klasifikasi Tumor Otak Div NeuroonkoDokument30 SeitenKlasifikasi Tumor Otak Div Neuroonkonovy rosalia chandraNoch keine Bewertungen
- Tumors of The CNSDokument26 SeitenTumors of The CNSShailendra Pratap SinghNoch keine Bewertungen
- Pinealglandtumors 141128232832 Conversion Gate01Dokument20 SeitenPinealglandtumors 141128232832 Conversion Gate01Mohammed FareedNoch keine Bewertungen
- PA 29 Testicular TumorsDokument46 SeitenPA 29 Testicular TumorsFangNoch keine Bewertungen
- Thyroid Neoplasm - Part 02 - Associate Prof DR Kishore G BanerjeeDokument24 SeitenThyroid Neoplasm - Part 02 - Associate Prof DR Kishore G Banerjeenaveenarageson4Noch keine Bewertungen
- DR - Ign Purna Putra, Sps (K)Dokument64 SeitenDR - Ign Purna Putra, Sps (K)Sheryl ElitaNoch keine Bewertungen
- Neoplasma Otak: FK UisuDokument32 SeitenNeoplasma Otak: FK UisuRifaMaisarohNoch keine Bewertungen
- Tumors of The Nervous SystemDokument6 SeitenTumors of The Nervous SystemRituNoch keine Bewertungen
- MeningiomaDokument7 SeitenMeningiomaLili HapverNoch keine Bewertungen
- Cranio Pha Ryn Gio MaDokument3 SeitenCranio Pha Ryn Gio MaSerious LeoNoch keine Bewertungen
- Brainstem Gliomas: BackgroundDokument10 SeitenBrainstem Gliomas: Backgroundanak99Noch keine Bewertungen
- Childhood Brain Tumors: Nabilah Binti Dato ' Ayob 060100814Dokument17 SeitenChildhood Brain Tumors: Nabilah Binti Dato ' Ayob 060100814NinaNoch keine Bewertungen
- The Radiology Assistant Brain Tumor - Systematic Approach PDFDokument29 SeitenThe Radiology Assistant Brain Tumor - Systematic Approach PDFMichael DeanNoch keine Bewertungen
- Brain Tumors: Primary BTDokument5 SeitenBrain Tumors: Primary BTMohamed Al-zichrawyNoch keine Bewertungen
- Tumors of The Nervous SystemDokument45 SeitenTumors of The Nervous SystemIsaac MwangiNoch keine Bewertungen
- Neoplasms of Childhood and Infancy: DR G Sirisha Assistant Professor Deparment of PathologyDokument25 SeitenNeoplasms of Childhood and Infancy: DR G Sirisha Assistant Professor Deparment of PathologyDevisriNoch keine Bewertungen
- Neuropathology: Dr. Siddaganga S MDokument29 SeitenNeuropathology: Dr. Siddaganga S Msiddaganga sigiNoch keine Bewertungen
- Tumors of Nervous SystemDokument50 SeitenTumors of Nervous SystemNininghrNoch keine Bewertungen
- Presented by Dr. Shamim Rima M.Phil Radiology & Imaging BsmmuDokument113 SeitenPresented by Dr. Shamim Rima M.Phil Radiology & Imaging Bsmmudr_shamimrNoch keine Bewertungen
- MCQS CNS PathologyDokument14 SeitenMCQS CNS PathologyFourth YearNoch keine Bewertungen
- Brain TumorDokument67 SeitenBrain TumorNur AgamiNoch keine Bewertungen
- Linee GuidaDokument7 SeitenLinee GuidaDPNoch keine Bewertungen
- Chest Wall TumorDokument27 SeitenChest Wall TumorRivani KurniawanNoch keine Bewertungen
- Normal Mediastinal Anatomy, Pathologies and Diagnostic MethodsDokument9 SeitenNormal Mediastinal Anatomy, Pathologies and Diagnostic MethodsJuma AwarNoch keine Bewertungen
- Oculars TumorDokument109 SeitenOculars TumorNovita EmyNoch keine Bewertungen
- Brain Tumors of ChildhoodDokument46 SeitenBrain Tumors of ChildhoodKirk08Noch keine Bewertungen
- Epidemiology and Pathology of Intraventricular TumorsDokument14 SeitenEpidemiology and Pathology of Intraventricular TumorsNaim CalilNoch keine Bewertungen
- Spinal Tumors - A Brief OverviewDokument38 SeitenSpinal Tumors - A Brief OverviewRAVIRAJ GHORPADE BELGAUM ADVANCED NEUROSURGERYNoch keine Bewertungen
- Intramedullary Spinal Cord TumorsDokument7 SeitenIntramedullary Spinal Cord TumorsmutalimNoch keine Bewertungen
- Soft Tissue TumorDokument248 SeitenSoft Tissue TumorDabessa MosissaNoch keine Bewertungen
- Thyroid GlandDokument81 SeitenThyroid Glanddr_shamimrNoch keine Bewertungen
- Bladder and Testis. PicDokument87 SeitenBladder and Testis. PicDr-Mohammad Ali-Fayiz Al TamimiNoch keine Bewertungen
- Fast Facts: Advanced Cutaneous Squamous Cell Carcinoma for Patients and their Supporters: Information + Taking Control = Best OutcomeVon EverandFast Facts: Advanced Cutaneous Squamous Cell Carcinoma for Patients and their Supporters: Information + Taking Control = Best OutcomeNoch keine Bewertungen
- A. Primary GlaucomaDokument5 SeitenA. Primary GlaucomasekiannNoch keine Bewertungen
- Definisi Shock, Klasifikasi Shock, Stadium ShockDokument8 SeitenDefinisi Shock, Klasifikasi Shock, Stadium ShocksekiannNoch keine Bewertungen
- Classification of NeuropathyDokument16 SeitenClassification of NeuropathysekiannNoch keine Bewertungen
- Transverse Myelitis: Differential DiagnosisDokument14 SeitenTransverse Myelitis: Differential DiagnosissekiannNoch keine Bewertungen
- LiverDokument20 SeitenLiversekiannNoch keine Bewertungen
- Ann Arbor Staging System For Hodgkin's DiseaseDokument3 SeitenAnn Arbor Staging System For Hodgkin's DiseasesekiannNoch keine Bewertungen
- Erythroplasia of QueyratDokument2 SeitenErythroplasia of QueyratsekiannNoch keine Bewertungen
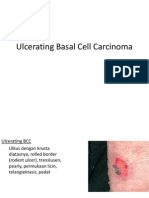
- Ulcerating Basal Cell CarcinomaDokument2 SeitenUlcerating Basal Cell CarcinomasekiannNoch keine Bewertungen
- Bowen's DiseaseDokument2 SeitenBowen's DiseasesekiannNoch keine Bewertungen
- Coordination - Human Bio HB10Dokument5 SeitenCoordination - Human Bio HB10Zah SchlafmützeNoch keine Bewertungen
- Kuliah 3. Biosintesis Dan Mekanisme Kerja Hormon Reproduksi PriaDokument38 SeitenKuliah 3. Biosintesis Dan Mekanisme Kerja Hormon Reproduksi PriaYulia Fatma NstNoch keine Bewertungen
- Special Senses WorksheetDokument5 SeitenSpecial Senses WorksheetEdison Alfonso SturgessNoch keine Bewertungen
- Lecture On The Histology of Cerebrum and Meninges by Dr. RoomiDokument20 SeitenLecture On The Histology of Cerebrum and Meninges by Dr. RoomiMudassar Roomi100% (1)
- Neurobiological Basis of Human BehaviorDokument72 SeitenNeurobiological Basis of Human Behaviorelvinegunawan0% (1)
- Basic of AutoimmunityDokument13 SeitenBasic of Autoimmunitymahadevabhu07100% (1)
- (Mebooksfree Net) Chr&kid&dis&dia&tre&yan&he&1st PDFDokument250 Seiten(Mebooksfree Net) Chr&kid&dis&dia&tre&yan&he&1st PDFmainoNoch keine Bewertungen
- PhysiologyDokument15 SeitenPhysiology221618Noch keine Bewertungen
- Cardiovascular System NotesDokument3 SeitenCardiovascular System NoteslemuelNoch keine Bewertungen
- BasicScienceYear10textbook PDFDokument133 SeitenBasicScienceYear10textbook PDFDove PaeaNoch keine Bewertungen
- Fulminant Hepatic Failure: Nattaphol UransilpDokument27 SeitenFulminant Hepatic Failure: Nattaphol UransilpChacha TasyaNoch keine Bewertungen
- Anatomy and Histology of The Cardiovascular SystemDokument16 SeitenAnatomy and Histology of The Cardiovascular SystemTasmiah HossainNoch keine Bewertungen
- PerfectionPeptide P3 201802Dokument25 SeitenPerfectionPeptide P3 201802NG Sze WingNoch keine Bewertungen
- Psychology Notes Units 1Dokument24 SeitenPsychology Notes Units 1Rohan Kaicker100% (1)
- Animal Tissue NotesDokument20 SeitenAnimal Tissue NotesSahejNoch keine Bewertungen
- The Twelve Tissue Salts (Cell Salts)Dokument3 SeitenThe Twelve Tissue Salts (Cell Salts)darlene918100% (2)
- Anatomy and Physiology of The Respiratory System (Handouts)Dokument5 SeitenAnatomy and Physiology of The Respiratory System (Handouts)bluecindy87Noch keine Bewertungen
- The Thyroid Reset Diet 3 ChaptersDokument71 SeitenThe Thyroid Reset Diet 3 ChaptersjovaneticNoch keine Bewertungen
- Cardiovascular AssessmentDokument13 SeitenCardiovascular AssessmentKathryn Bianca AcanceNoch keine Bewertungen
- Curs 15v-2018hDokument96 SeitenCurs 15v-2018hMirceaDraghiciNoch keine Bewertungen
- Why Is It Necessary For The Trachea To Have Rings of Cartilage in Its WallsDokument3 SeitenWhy Is It Necessary For The Trachea To Have Rings of Cartilage in Its Wallsapi-265276766Noch keine Bewertungen
- Poorly Differentiated Thyroid CarcinomaDokument67 SeitenPoorly Differentiated Thyroid Carcinomaperie_md100% (1)
- Cardiovascular System - Heart IntroDokument6 SeitenCardiovascular System - Heart IntroKate Angeline TanNoch keine Bewertungen
- Anterior and Posterio Pituitary GlandDokument7 SeitenAnterior and Posterio Pituitary GlandAnny AlvrzNoch keine Bewertungen
- Nutritional Foundations and Clinical Applications 5th Edition Grodner Test BankDokument10 SeitenNutritional Foundations and Clinical Applications 5th Edition Grodner Test BankKareemNoch keine Bewertungen
- Week 14 - OBF Analysis (Gastric Fluid)Dokument19 SeitenWeek 14 - OBF Analysis (Gastric Fluid)Astrud LabradorNoch keine Bewertungen
- McMinn's Concise Human Anatomy 2nd EdDokument289 SeitenMcMinn's Concise Human Anatomy 2nd Edica ssNoch keine Bewertungen
- The Sequence of Events That Occur in The Heart During Cardiac CycleDokument13 SeitenThe Sequence of Events That Occur in The Heart During Cardiac CycleADITYAROOP PATHAKNoch keine Bewertungen
- Anatomy & Physiology of Olfactory System.Dokument27 SeitenAnatomy & Physiology of Olfactory System.Prasanna DattaNoch keine Bewertungen
- Kab ReetDokument254 SeitenKab ReetAsia AlhkeemNoch keine Bewertungen