Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- A Mineral Job Application: Human Body Co. Metabolic Unit ApplicationDokument3 SeitenA Mineral Job Application: Human Body Co. Metabolic Unit ApplicationTimothy Mar100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Post TestDokument9 SeitenPost TestPradnya Paramitha100% (2)
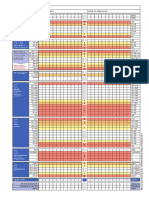
- NEWS2 Chart 3 - NEWS Observation Chart - 0 PDFDokument1 SeiteNEWS2 Chart 3 - NEWS Observation Chart - 0 PDFFlouria Stefanny SimatupangNoch keine Bewertungen
- ITLS 8e Advanced Post Test Exam Version BDokument10 SeitenITLS 8e Advanced Post Test Exam Version BMohamed TabanaNoch keine Bewertungen
- Case Study - Diabetes Mellitus (Nutrition&Dietetics)Dokument10 SeitenCase Study - Diabetes Mellitus (Nutrition&Dietetics)Summer Suarez100% (1)
- Nursing Management of A Patient With An Ectopic PregnancyDokument8 SeitenNursing Management of A Patient With An Ectopic PregnancySummer SuarezNoch keine Bewertungen
- NCP2 - DengueDokument4 SeitenNCP2 - DengueSummer SuarezNoch keine Bewertungen
- Nursing Management of Patient With Community Acquired PneumoniaDokument5 SeitenNursing Management of Patient With Community Acquired PneumoniaSummer SuarezNoch keine Bewertungen
- NCP2 - Acute PainDokument2 SeitenNCP2 - Acute PainSummer SuarezNoch keine Bewertungen
- NCP (Afp)Dokument7 SeitenNCP (Afp)Summer SuarezNoch keine Bewertungen
- A Diagnostic Tool That Measures and Records The Electrical Activity of The Heart. - ECG Is Recorded by Applying Electrodes and Connecting Them To A Recording ApparatusDokument12 SeitenA Diagnostic Tool That Measures and Records The Electrical Activity of The Heart. - ECG Is Recorded by Applying Electrodes and Connecting Them To A Recording ApparatusSummer SuarezNoch keine Bewertungen
- Drug Study (AFP)Dokument10 SeitenDrug Study (AFP)Summer SuarezNoch keine Bewertungen
- Generic Name Indication Action Contraindication Adverse Reaction Nursing ConsiderationDokument8 SeitenGeneric Name Indication Action Contraindication Adverse Reaction Nursing ConsiderationSummer SuarezNoch keine Bewertungen
- FNCPDokument1 SeiteFNCPSummer SuarezNoch keine Bewertungen
- FNCPDokument1 SeiteFNCPSummer SuarezNoch keine Bewertungen
- Light Independent ReactionDokument10 SeitenLight Independent ReactionazwelljohnsonNoch keine Bewertungen
- Blood Pressure Automatic: Intelli SenseDokument2 SeitenBlood Pressure Automatic: Intelli SenseDnGNoch keine Bewertungen
- Erythropoiesis: Definition Site of ErythropoiesisDokument6 SeitenErythropoiesis: Definition Site of ErythropoiesisAnusuya SNoch keine Bewertungen
- Topic 7: Respiration, Muscles and The Internal Environment Chapter 7A: Cellular RespirationDokument3 SeitenTopic 7: Respiration, Muscles and The Internal Environment Chapter 7A: Cellular RespirationsalmaNoch keine Bewertungen
- Topic 1 Endocrine SystemDokument140 SeitenTopic 1 Endocrine SystemmasdfgNoch keine Bewertungen
- Photosynthesis & LeavesDokument38 SeitenPhotosynthesis & LeavesSanthoshNoch keine Bewertungen
- T P R B P: Vital SignsDokument20 SeitenT P R B P: Vital SignsEla 15Noch keine Bewertungen
- AUTOPSY ReezuDokument16 SeitenAUTOPSY ReezuBnB UsmleNoch keine Bewertungen
- Chapter 26 Dysrhythmias Quizlet 1Dokument5 SeitenChapter 26 Dysrhythmias Quizlet 1Marshin Thea CelociaNoch keine Bewertungen
- EKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture SeriesDokument85 SeitenEKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture Seriesandina rosmalianti100% (1)
- Renal Physiology Equations: C U) V P) Excretionrate Serum Concentration C C GFRDokument3 SeitenRenal Physiology Equations: C U) V P) Excretionrate Serum Concentration C C GFRJoão Batista Lopes CostaNoch keine Bewertungen
- GB1 Q2 TosDokument2 SeitenGB1 Q2 TosRuby UriarteNoch keine Bewertungen
- Li Et Al 2003Dokument6 SeitenLi Et Al 2003Adrian McDoucheNoch keine Bewertungen
- ECG Facut de MineDokument3 SeitenECG Facut de MineKing Bal94Noch keine Bewertungen
- Darah Dan Fungsi DarahDokument14 SeitenDarah Dan Fungsi DarahdelisNoch keine Bewertungen
- Nursing Care PlanDokument2 SeitenNursing Care PlanRachelleNoch keine Bewertungen
- Case Study Burn InjuryDokument9 SeitenCase Study Burn InjuryAmber Dawn MonteroNoch keine Bewertungen
- Acute Severe Asthma (Status Asthmaticus)Dokument20 SeitenAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNoch keine Bewertungen
- LP 1.2 in PhysioBio PsychologyDokument11 SeitenLP 1.2 in PhysioBio PsychologyWayne GodioNoch keine Bewertungen
- Human Physiology in An Aquatic EnvironmentDokument47 SeitenHuman Physiology in An Aquatic EnvironmentMARIA CAMILA RENGIFO CAICEDONoch keine Bewertungen
- Lesson Biological OrganizationDokument49 SeitenLesson Biological OrganizationReinalyn MendozaNoch keine Bewertungen
- Secondary MessengerDokument50 SeitenSecondary MessengerFlorlin Grace YradNoch keine Bewertungen
- Cardiac OutputDokument61 SeitenCardiac OutputSyed Ali MoosaNoch keine Bewertungen
- Biology Chapter 8 (Due Jan. 18, Test Jan. 22)Dokument9 SeitenBiology Chapter 8 (Due Jan. 18, Test Jan. 22)عبدالرحمن شحاتهNoch keine Bewertungen
- Plant Tissues: Class: 7 Board: ICSE Year: 2021-2022Dokument31 SeitenPlant Tissues: Class: 7 Board: ICSE Year: 2021-2022shalu malaniNoch keine Bewertungen
- Tracing:: ABILLAR, Rica MendozaDokument2 SeitenTracing:: ABILLAR, Rica Mendozajzyryl abillarNoch keine Bewertungen