Das könnte Ihnen auch gefallen
- Muscle Up PDFDokument7 SeitenMuscle Up PDFJan Zejdlik0% (2)
- CXR Lecture DR Lenora FernandezDokument70 SeitenCXR Lecture DR Lenora Fernandezapi-19431894100% (1)
- Programming For Athletic PerformanceDokument7 SeitenProgramming For Athletic Performancemike100% (2)
- Altered Mental StatusDokument151 SeitenAltered Mental StatusbrentupdegraffNoch keine Bewertungen
- Approach To Chest PainDokument52 SeitenApproach To Chest PainChris Jardine LiNoch keine Bewertungen
- Anaesthesia SummaryDokument36 SeitenAnaesthesia SummaryRazan QassemNoch keine Bewertungen
- EkgDokument94 SeitenEkgCaprita LauraNoch keine Bewertungen
- Transporting Critically Ill PatientsDokument48 SeitenTransporting Critically Ill PatientsRichard GunawanNoch keine Bewertungen
- Rapid Interpretation of EcgsDokument41 SeitenRapid Interpretation of EcgsAdela abboudNoch keine Bewertungen
- Newborn EmergenciesDokument83 SeitenNewborn EmergencieshwelpNoch keine Bewertungen
- Introduction of CRRT 2006Dokument25 SeitenIntroduction of CRRT 2006yamtotlNoch keine Bewertungen
- Intrahospital Transport of Critically Ill PatientsDokument14 SeitenIntrahospital Transport of Critically Ill Patientsعزالدين الزوقريNoch keine Bewertungen
- Monitoring OF Hemorrhagic Shock: Basrul HanafiDokument24 SeitenMonitoring OF Hemorrhagic Shock: Basrul HanafiabdurrahmanNoch keine Bewertungen
- Management of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaDokument77 SeitenManagement of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaAETCM Emergency medicineNoch keine Bewertungen
- Pass Critical Care Endocrine Frcem ResourcesDokument41 SeitenPass Critical Care Endocrine Frcem ResourcesYoussef SaadNoch keine Bewertungen
- Ekg Normal Dan Acs Sudin TimurDokument59 SeitenEkg Normal Dan Acs Sudin TimurArum MaharaniNoch keine Bewertungen
- Mechanical Ventilation and Intracranial PressureDokument30 SeitenMechanical Ventilation and Intracranial PressureFlavius AnghelNoch keine Bewertungen
- The QT Interval PDFDokument4 SeitenThe QT Interval PDFFeliciaSetiawanNoch keine Bewertungen
- Manuel Utilisateur Holters 3 Parametres GIMA (Anglais)Dokument56 SeitenManuel Utilisateur Holters 3 Parametres GIMA (Anglais)Crios MNoch keine Bewertungen
- Principles of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDokument117 SeitenPrinciples of Antibiotics: Deepa V Post Graduate Student DSCDS, BangaloreDeepa VenkateshNoch keine Bewertungen
- Emergency Lecture PDFDokument57 SeitenEmergency Lecture PDFDuane Liloc100% (1)
- Abg Made EasyDokument24 SeitenAbg Made EasynbvillarazoNoch keine Bewertungen
- Basic Practice of Anesthesiology FinalDokument70 SeitenBasic Practice of Anesthesiology FinalAfiqah So JasmiNoch keine Bewertungen
- Ventricular ArrhytmiaDokument30 SeitenVentricular ArrhytmiaIkhsan AmadeaNoch keine Bewertungen
- Cardiovascular Disorders 1Dokument44 SeitenCardiovascular Disorders 1Nader Smadi100% (1)
- Notes For Clincal CasesDokument12 SeitenNotes For Clincal CasesMandeepNoch keine Bewertungen
- Intracardiac PressuresDokument41 SeitenIntracardiac Pressureswaleed315Noch keine Bewertungen
- PAC and Hemodynamic Monitoring 2-4-08Dokument32 SeitenPAC and Hemodynamic Monitoring 2-4-08anum786110Noch keine Bewertungen
- Peds Handbook 2017 - 2018Dokument25 SeitenPeds Handbook 2017 - 2018Michael MangubatNoch keine Bewertungen
- Neurologic Emergencies Stroke & Tia: Devin R. Harris, MD MHSC CCFP (Em)Dokument10 SeitenNeurologic Emergencies Stroke & Tia: Devin R. Harris, MD MHSC CCFP (Em)Samantha Lui100% (2)
- Chapter 1 - Central Venous CathetersDokument6 SeitenChapter 1 - Central Venous CathetersParth PatelNoch keine Bewertungen
- Intubations Outside ICUDokument79 SeitenIntubations Outside ICUzulham effendyNoch keine Bewertungen
- Wallenberg Syndrome: Publication DetailsDokument9 SeitenWallenberg Syndrome: Publication DetailsHuang Jen Liang100% (1)
- CCU Clinical GuidelinesDokument63 SeitenCCU Clinical GuidelinesHAMMYER ALROKHAMINoch keine Bewertungen
- Procedural Sedation - Audit Information 2017-18Dokument14 SeitenProcedural Sedation - Audit Information 2017-18Anonymous msnwfNd0% (1)
- ECG - ACLS 2020 ModuleDokument68 SeitenECG - ACLS 2020 ModuleRasheedAladdinNGuiomala100% (1)
- Lecture 4: Hypovolemic ShockDokument20 SeitenLecture 4: Hypovolemic Shockj.doe.hex_87Noch keine Bewertungen
- Understanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDokument52 SeitenUnderstanding Mechanical Ventilation: Jennifer Zanni, PT, DSCPT Johns Hopkins HospitalDeepa BhattacharjeeNoch keine Bewertungen
- Approach To PoisoningDokument107 SeitenApproach To PoisoningAlex beharuNoch keine Bewertungen
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDokument112 SeitenOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNoch keine Bewertungen
- Inferior Wall ST Elevation (STEMI)Dokument46 SeitenInferior Wall ST Elevation (STEMI)Hendrik100% (1)
- Microcirculation as Related to ShockVon EverandMicrocirculation as Related to ShockDavid SheproNoch keine Bewertungen
- Journal ClubDokument26 SeitenJournal Clubysindhura23gmailcom100% (1)
- Cardiovascular EmergenciesDokument20 SeitenCardiovascular EmergenciesJohn FisherNoch keine Bewertungen
- Rapid Sequence Intubation and Cricoid PressureDokument16 SeitenRapid Sequence Intubation and Cricoid PressureErlin IrawatiNoch keine Bewertungen
- Normal Impulse Conduction: Sinoatrial NodeDokument80 SeitenNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- Rhythm Packet: Normal ECG CriteriaDokument19 SeitenRhythm Packet: Normal ECG CriteriaRegina MithaNoch keine Bewertungen
- Infection in Critical CareDokument34 SeitenInfection in Critical CareSuresh Kumar BansalNoch keine Bewertungen
- Intra Aortic Balloon PumpDokument3 SeitenIntra Aortic Balloon PumpNkk Aqnd MgdnglNoch keine Bewertungen
- Basics of Ventilatory SupportDokument43 SeitenBasics of Ventilatory SupportAdhithya Bhat100% (1)
- Acls 2015Dokument9 SeitenAcls 2015Andy PrasetyoNoch keine Bewertungen
- Welcome: ACLS Course Will Start ShortlyDokument148 SeitenWelcome: ACLS Course Will Start ShortlyIan Orwa100% (1)
- Initiating of Mechanical Ventilation 7-3-10Dokument38 SeitenInitiating of Mechanical Ventilation 7-3-10KrysnaNoch keine Bewertungen
- Emtyazology 2nd ED 2015 مفهرس.WhiteKnightLove PDFDokument426 SeitenEmtyazology 2nd ED 2015 مفهرس.WhiteKnightLove PDFashrafasd100% (2)
- Learning Station 4 Toxicologic Emergencies: ©1999 American Heart AssociationDokument59 SeitenLearning Station 4 Toxicologic Emergencies: ©1999 American Heart AssociationbrentupdegraffNoch keine Bewertungen
- 8.the Atls ProtocolDokument57 Seiten8.the Atls ProtocolReuben DutiNoch keine Bewertungen
- Fluid Resuscitation - Dita AditianingsihDokument48 SeitenFluid Resuscitation - Dita AditianingsihGalih Wicaksono100% (1)
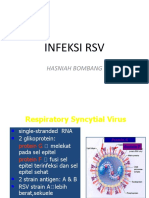
- Infeksi RSV: Hasniah BombangDokument12 SeitenInfeksi RSV: Hasniah Bombangmuh hardiansyahNoch keine Bewertungen
- Disease Mechanism of Action NoteDokument3 SeitenDisease Mechanism of Action Noteamoody95Noch keine Bewertungen
- Ap Psychology Group Project MotivationDokument1 SeiteAp Psychology Group Project Motivationapi-333631531Noch keine Bewertungen
- Chts Girls PDokument15 SeitenChts Girls PIkram KundiNoch keine Bewertungen
- 30 Nutrition MythsDokument218 Seiten30 Nutrition MythsBeatrice Caitanu67% (3)
- Alcohols, Diols, TriolsDokument32 SeitenAlcohols, Diols, TriolsShivam GuptaNoch keine Bewertungen
- Assessing The AbdomenDokument18 SeitenAssessing The Abdomenmartinezrose32Noch keine Bewertungen
- Food and Nutrition Jean DrezeDokument7 SeitenFood and Nutrition Jean DrezeSamridh NangiaNoch keine Bewertungen
- P90X ScheduleDokument8 SeitenP90X Scheduleh0stilityNoch keine Bewertungen
- Testbank 4e ch16Dokument13 SeitenTestbank 4e ch16drnazz100% (9)
- Health Awareness EssayDokument2 SeitenHealth Awareness EssayDrake SmithNoch keine Bewertungen
- The Effect of Fast FoodDokument1 SeiteThe Effect of Fast FoodQinthara Alifya PNoch keine Bewertungen
- 6 Things Before Starting A DietDokument2 Seiten6 Things Before Starting A DietLUMINITA GIUCANoch keine Bewertungen
- Unit 5 Class Audio ScriptsDokument22 SeitenUnit 5 Class Audio ScriptsskilachNoch keine Bewertungen
- Orms Nutrition Plan RealDokument3 SeitenOrms Nutrition Plan Realapi-336639469Noch keine Bewertungen
- Key of SEQsDokument5 SeitenKey of SEQsMudassar RoomiNoch keine Bewertungen
- Ischemic Heart DiseaseDokument47 SeitenIschemic Heart DiseaseAbood SamoudiNoch keine Bewertungen
- EndocrinologyDokument23 SeitenEndocrinologysaikat55Noch keine Bewertungen
- 90 DaysDokument272 Seiten90 DayspamlotoNoch keine Bewertungen
- Fast Food RestaurantDokument19 SeitenFast Food RestaurantVivek GyawaliNoch keine Bewertungen
- A Healthy Diet British English Teacher Ver2 BWDokument4 SeitenA Healthy Diet British English Teacher Ver2 BWDaniel BourneNoch keine Bewertungen
- Nonalcoholic Fatty Liver Disease (Nafld) Challenge To DiagnosisDokument31 SeitenNonalcoholic Fatty Liver Disease (Nafld) Challenge To DiagnosisMohamed NaguibNoch keine Bewertungen
- The Right Weight: Matters! Matters! Matters!Dokument1 SeiteThe Right Weight: Matters! Matters! Matters!Hartford CourantNoch keine Bewertungen
- IntroductionDokument4 SeitenIntroductionCristina L. JaysonNoch keine Bewertungen
- AdiposeDokument31 SeitenAdiposeCzarina David100% (1)
- ACE Inhibitors Vs ARBsDokument4 SeitenACE Inhibitors Vs ARBsRizqi Haqqum MNoch keine Bewertungen
- Delayed TransformationDokument5 SeitenDelayed Transformationenigmaticthinking100% (1)
- Case Study CVDDokument8 SeitenCase Study CVDChloe AguiNoch keine Bewertungen
- Bio+306 03+cholesterol+determination+in+serumDokument14 SeitenBio+306 03+cholesterol+determination+in+serumDawlat SalamaNoch keine Bewertungen
- Jurnal 5 - Meisya Nur'aini - 22030118130064Dokument5 SeitenJurnal 5 - Meisya Nur'aini - 22030118130064Meisya Nur'ainiNoch keine Bewertungen