Das könnte Ihnen auch gefallen
- Neuro tract lesions guide for UMN, LMN deficitsDokument16 SeitenNeuro tract lesions guide for UMN, LMN deficitsসোমনাথ মহাপাত্রNoch keine Bewertungen
- Stroke School Brockville Part 3Dokument39 SeitenStroke School Brockville Part 3Gautam KhannaNoch keine Bewertungen
- Cranial Nerve Examination: A Step-by-Step GuideDokument45 SeitenCranial Nerve Examination: A Step-by-Step GuideTanat AsavisanuNoch keine Bewertungen
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisVon EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisBewertung: 5 von 5 Sternen5/5 (1)
- Neurology Multiple Choice Questions With Explanations: Volume IVon EverandNeurology Multiple Choice Questions With Explanations: Volume IBewertung: 4 von 5 Sternen4/5 (7)
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesVon EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNoch keine Bewertungen
- Aicardi’s Diseases of the Nervous System in Childhood, 4th EditionVon EverandAicardi’s Diseases of the Nervous System in Childhood, 4th EditionAlexis ArzimanoglouNoch keine Bewertungen
- Neurology Multiple Choice Questions With Explanations: Volume IIVon EverandNeurology Multiple Choice Questions With Explanations: Volume IIBewertung: 5 von 5 Sternen5/5 (2)
- Syncope, A Simple Guide to the Condition, Treatment and Related DiseasesVon EverandSyncope, A Simple Guide to the Condition, Treatment and Related DiseasesNoch keine Bewertungen
- Stroke FullDokument10 SeitenStroke Fullshowkat3Noch keine Bewertungen
- Cerebrum Sulci and Gyri and Circle of WillisDokument53 SeitenCerebrum Sulci and Gyri and Circle of Willisgandhiayu100% (1)
- Neurology Short NotesDokument11 SeitenNeurology Short NotesSachin Kumar Rastogi100% (1)
- Blood Supply of The BrainDokument37 SeitenBlood Supply of The BrainueumanaNoch keine Bewertungen
- Stroke Syndromes and Localization 2007Dokument56 SeitenStroke Syndromes and Localization 2007SaintPaul Univ100% (1)
- Pons MedullaDokument32 SeitenPons MedullaEnaWahahaNoch keine Bewertungen
- Neuro LesionsDokument7 SeitenNeuro Lesionskep1313100% (5)
- Descending Tracts: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, TumkurDokument23 SeitenDescending Tracts: Dr. Niranjan Murthy H L Asst Prof of Physiology SSMC, Tumkurnirilib100% (1)
- Peripheral Nerve Injury: J. Navin KumarDokument100 SeitenPeripheral Nerve Injury: J. Navin Kumarpuravi91Noch keine Bewertungen
- Nerve TractsDokument38 SeitenNerve TractsAbualauon AlbeblawyNoch keine Bewertungen
- Cardiac MurmursDokument53 SeitenCardiac MurmursdrgashokNoch keine Bewertungen
- 35ekg 1Dokument103 Seiten35ekg 1Veerapong Vattanavanit100% (2)
- NeuroTracts - Ascending, Descending, UMN, LMNDokument5 SeitenNeuroTracts - Ascending, Descending, UMN, LMNBrandi Allen HensonNoch keine Bewertungen
- Common Histories and Red Flags Presentation Noninteractive VersionDokument21 SeitenCommon Histories and Red Flags Presentation Noninteractive VersionesmarNoch keine Bewertungen
- UMass Medical School Mind Brain Behavior 1 Spinal Cord Atlas OverviewDokument11 SeitenUMass Medical School Mind Brain Behavior 1 Spinal Cord Atlas Overviewnon_zense100% (1)
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDokument6 SeitenHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNoch keine Bewertungen
- MnemonicsDokument254 SeitenMnemonicsMuhammad Rahim ArshadNoch keine Bewertungen
- PRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewDokument5 SeitenPRES (Posterior Reversible Encephalopathy Syndrome) and Eclampsia-ReviewAvicena M IqbalNoch keine Bewertungen
- VALVULAR HEART DISEASE GUIDEDokument69 SeitenVALVULAR HEART DISEASE GUIDEAbanoub AwadallaNoch keine Bewertungen
- Leukodystrophy Presentations and Testing GuideDokument43 SeitenLeukodystrophy Presentations and Testing GuideFabio Giacalone100% (1)
- Cardiology A. Woo PDFDokument52 SeitenCardiology A. Woo PDFiuliNoch keine Bewertungen
- SMP Neuro Lab ManualDokument37 SeitenSMP Neuro Lab Manualsas345sas345Noch keine Bewertungen
- Blood Suppy of BrainDokument54 SeitenBlood Suppy of BrainZoya MoraniNoch keine Bewertungen
- Neuroscience Clerkship Teaching Vignettes on Cerebrovascular Disease and Changes in Mental StateDokument16 SeitenNeuroscience Clerkship Teaching Vignettes on Cerebrovascular Disease and Changes in Mental Statehippocamper100% (1)
- Neurology Shelf Exam Review - Part 2.newDokument14 SeitenNeurology Shelf Exam Review - Part 2.newyogurtNoch keine Bewertungen
- Basal GangliaDokument29 SeitenBasal Gangliaapi-19916399Noch keine Bewertungen
- HypocalcemiaDokument23 SeitenHypocalcemiarayrrn00Noch keine Bewertungen
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDokument45 SeitenHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801Noch keine Bewertungen
- Cardiology MnemonicsDokument12 SeitenCardiology MnemonicsEliza SparkNoch keine Bewertungen
- X-Ray CVSDokument67 SeitenX-Ray CVSmdjohariNoch keine Bewertungen
- พี่พงษ์ติวcardioDokument79 Seitenพี่พงษ์ติวcardioRapid Medicine67% (3)
- Neurology MnemonicsDokument2 SeitenNeurology MnemonicsJan Taplin100% (1)
- Anatomy of The Thorax (CT)Dokument7 SeitenAnatomy of The Thorax (CT)darmariantoNoch keine Bewertungen
- CT in Head TraumaDokument4 SeitenCT in Head TraumasunguramjanjaNoch keine Bewertungen
- Approach To Neurological DiseaseDokument68 SeitenApproach To Neurological DiseaseNEuRoLoGisT CoFFeeCuPNoch keine Bewertungen
- Cardiology Cardiovascular: Aortic Stenosis CharacteristicsDokument11 SeitenCardiology Cardiovascular: Aortic Stenosis CharacteristicsxaileenxNoch keine Bewertungen
- Renal OsteodystrophyDokument4 SeitenRenal OsteodystrophyLuigiNoch keine Bewertungen
- (MicroB) 3.6 Brainstem LesionsDokument6 Seiten(MicroB) 3.6 Brainstem Lesionsnelson lopezNoch keine Bewertungen
- General Chemistry: Hematology Values Red Blood Cell ValuesDokument2 SeitenGeneral Chemistry: Hematology Values Red Blood Cell ValuesDanica ZaragozaNoch keine Bewertungen
- NeuroradiologyDokument11 SeitenNeuroradiologysarguss14100% (2)
- Approach To A Patient With HemiplegiaDokument4 SeitenApproach To A Patient With Hemiplegiajslum100% (4)
- MCTDDokument36 SeitenMCTDRapid Medicine100% (1)
- StrokeDokument66 SeitenStrokeJoshua Smith100% (1)
- Lesion Localization in NeurologyDokument34 SeitenLesion Localization in NeurologyValeria Leon AbadNoch keine Bewertungen
- Anatomy and Physiology of BrainDokument21 SeitenAnatomy and Physiology of BrainNavjot BrarNoch keine Bewertungen
- Mnemonics For Medical PGEntranceDokument145 SeitenMnemonics For Medical PGEntranceCharan RebelNoch keine Bewertungen
- Mitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationDokument33 SeitenMitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationcafemedNoch keine Bewertungen
- Group 5 project on oxygen properties and applicationsDokument11 SeitenGroup 5 project on oxygen properties and applicationsAngga SaputraNoch keine Bewertungen
- SirsDokument33 SeitenSirsBinod Bade ShresthaNoch keine Bewertungen
- Bulgarian Split Squat Lateral: Lateral LungeDokument47 SeitenBulgarian Split Squat Lateral: Lateral LungeZac Brouillette100% (10)
- How To Analyze EkgsDokument40 SeitenHow To Analyze EkgsJosh WeisNoch keine Bewertungen
- MODULE 1 & 2 - General Biology 2Dokument12 SeitenMODULE 1 & 2 - General Biology 2John Michael LopezNoch keine Bewertungen
- FSBGD MCQ Study Questions 2001Dokument84 SeitenFSBGD MCQ Study Questions 2001api-2629165192% (12)
- First Aid, Survival, and CPR Home and Field Pocket GuideDokument243 SeitenFirst Aid, Survival, and CPR Home and Field Pocket Guideantonakis69100% (5)
- TCM PDFDokument435 SeitenTCM PDFalintuta2Noch keine Bewertungen
- Stewart Bitkoff - StarchildDokument9 SeitenStewart Bitkoff - StarchildSat FeedNoch keine Bewertungen
- 148604-Care Path MENTAL STATUS CHANGE v10 PDFDokument1 Seite148604-Care Path MENTAL STATUS CHANGE v10 PDFAnonymous 8qVcBze8qNoch keine Bewertungen
- Tracking Genetically-Engineered Microorganisms (Biotechnology Intelligence Unit)Dokument178 SeitenTracking Genetically-Engineered Microorganisms (Biotechnology Intelligence Unit)Fabio LimaNoch keine Bewertungen
- Weekly Home Learning Plan: Department of EducationDokument19 SeitenWeekly Home Learning Plan: Department of EducationMaya CondeNoch keine Bewertungen
- Terminologi Kedokteran - LEGDokument51 SeitenTerminologi Kedokteran - LEGAmira SyahabNoch keine Bewertungen
- Cor Pulmonale - StatPearls - NCBI BookshelfDokument4 SeitenCor Pulmonale - StatPearls - NCBI BookshelfAldi RafaelNoch keine Bewertungen
- Lesson 4-Communication ModelsDokument19 SeitenLesson 4-Communication ModelsChristine Mae MontesNoch keine Bewertungen
- General Zoology-Midterm ReviewerDokument5 SeitenGeneral Zoology-Midterm ReviewerELIZA NICOLE ATANoch keine Bewertungen
- Nanoelectromechanical Systems: Condensed Matter Physics 114-36, California Institute of Technology Pasadena, CA 91125Dokument19 SeitenNanoelectromechanical Systems: Condensed Matter Physics 114-36, California Institute of Technology Pasadena, CA 91125Yash SakujaNoch keine Bewertungen
- BehaviorismDokument22 SeitenBehaviorismOlcay Sanem SipahioğluNoch keine Bewertungen
- Flowering Plant MorphologyDokument513 SeitenFlowering Plant MorphologyVaibhav PanchalNoch keine Bewertungen
- 2nd Lab Depex ReviewerDokument46 Seiten2nd Lab Depex ReviewerprincelfangorNoch keine Bewertungen
- Year 4 Science Learner's BookDokument106 SeitenYear 4 Science Learner's BookFatme AllawaNoch keine Bewertungen
- ProArgi-9 Plus Fact SheetDokument1 SeiteProArgi-9 Plus Fact SheetuksynergyNoch keine Bewertungen
- Cell AnalogyDokument2 SeitenCell AnalogyVea Ann CantollasNoch keine Bewertungen
- BBO 2011 Round 2Dokument16 SeitenBBO 2011 Round 2martynapetNoch keine Bewertungen
- GR 173259Dokument11 SeitenGR 173259Anonymous wDganZNoch keine Bewertungen
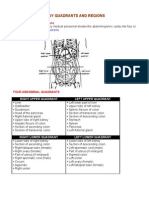
- Organs in The Body Quadrants and RegionsDokument3 SeitenOrgans in The Body Quadrants and RegionsDavid HosamNoch keine Bewertungen
- DPP - Anatomy of Flowering PlantsDokument10 SeitenDPP - Anatomy of Flowering PlantsRitika GochhaitNoch keine Bewertungen
- New England Journal Medicine: The ofDokument11 SeitenNew England Journal Medicine: The ofnenda nurfendaNoch keine Bewertungen
- The 4 Main Types of Animal Tissues and Their FunctionsDokument16 SeitenThe 4 Main Types of Animal Tissues and Their FunctionsMithu VarshaNoch keine Bewertungen
- IPPA Procedures Guide for Nursing StudentsDokument5 SeitenIPPA Procedures Guide for Nursing StudentsJulieeNoch keine Bewertungen