Das könnte Ihnen auch gefallen
- Expressions of the Mind in Words: Writings by a 9 year old kidVon EverandExpressions of the Mind in Words: Writings by a 9 year old kidNoch keine Bewertungen
- Autism and Abnormalities in The BrainDokument9 SeitenAutism and Abnormalities in The BrainAlan Challoner100% (1)
- How Healthy Are We?: A National Study of Well-Being at MidlifeVon EverandHow Healthy Are We?: A National Study of Well-Being at MidlifeNoch keine Bewertungen
- Students' MetacognitiveDokument11 SeitenStudents' MetacognitiveMicheal LezondraNoch keine Bewertungen
- Differential Diagnosis: Narcissistic Personality DisorderDokument4 SeitenDifferential Diagnosis: Narcissistic Personality DisorderBob ShaferNoch keine Bewertungen
- The Bullring: A Classroom Experiment in Moral EducationVon EverandThe Bullring: A Classroom Experiment in Moral EducationNoch keine Bewertungen
- Savant Skills Fact SheetDokument7 SeitenSavant Skills Fact SheetgabreNoch keine Bewertungen
- The Effectiveness of RAADS-R As A Screening Tool FDokument6 SeitenThe Effectiveness of RAADS-R As A Screening Tool FCarola ValdésNoch keine Bewertungen
- Carly Voice Breaking Through Autism 470467 PDFDokument6 SeitenCarly Voice Breaking Through Autism 470467 PDFFederico DcfNoch keine Bewertungen
- CC SR ProjectDokument11 SeitenCC SR Projectapi-617045311100% (1)
- Parent Child Bed SharingDokument24 SeitenParent Child Bed SharingquinhoxNoch keine Bewertungen
- Psychological DisordersDokument8 SeitenPsychological DisordersDenise NicoleNoch keine Bewertungen
- Dementia NICE GuidelinesDokument58 SeitenDementia NICE GuidelinesHardeep Singh BaliNoch keine Bewertungen
- Specific Developmental DisorderDokument41 SeitenSpecific Developmental DisorderKarthik SathyanNoch keine Bewertungen
- 1001 Great Ideas For Teaching and Raising Children With Autism or Asperger's - Ellen Notbohm, Veronica ZyskDokument1.312 Seiten1001 Great Ideas For Teaching and Raising Children With Autism or Asperger's - Ellen Notbohm, Veronica ZyskTijana Brzić0% (1)
- Bullying We Can All Help Stop ItDokument8 SeitenBullying We Can All Help Stop ItHRCNoch keine Bewertungen
- Recognizing and Understanding Schizophrenia in Young AdultsDokument31 SeitenRecognizing and Understanding Schizophrenia in Young AdultsInternational Medical Publisher100% (3)
- Micro Finance Services For Very Poor People - Promising Approaches From The FieldDokument16 SeitenMicro Finance Services For Very Poor People - Promising Approaches From The FieldPoverty Outreach Working Group (POWG)Noch keine Bewertungen
- False Memory SyndromeDokument6 SeitenFalse Memory SyndromeZainab MansoorNoch keine Bewertungen
- Psych 575 Disorder PSYCH 575 WEEK 5 DISORDER PAPER Select A Neurological, Psychological, or Neurodevelopmental Disorder. THE DISORDER FOR THIS PAPER IS PARKINSON'S DIESESEDokument13 SeitenPsych 575 Disorder PSYCH 575 WEEK 5 DISORDER PAPER Select A Neurological, Psychological, or Neurodevelopmental Disorder. THE DISORDER FOR THIS PAPER IS PARKINSON'S DIESESEWrite This Way (R)100% (1)
- By Hamra Faris.: in ChildhoodDokument18 SeitenBy Hamra Faris.: in ChildhoodhamrafarisNoch keine Bewertungen
- LIST OF PHOBIAS (Assignment in Psycho)Dokument70 SeitenLIST OF PHOBIAS (Assignment in Psycho)Eli Joshua EvangelistaNoch keine Bewertungen
- Mental Disorders WHO 2020Dokument6 SeitenMental Disorders WHO 2020BeatrizNoch keine Bewertungen
- DSM 5 Specific Learning Disorder Fact SheetDokument2 SeitenDSM 5 Specific Learning Disorder Fact SheetAnonymous Pj6Odj0% (1)
- Denver Developmental Screening TestDokument8 SeitenDenver Developmental Screening TestEleanor AlmendralNoch keine Bewertungen
- TrichotillamaniaDokument10 SeitenTrichotillamaniaTaraNoch keine Bewertungen
- Pervasive Developmental Disorders - Indian SceneDokument11 SeitenPervasive Developmental Disorders - Indian SceneVijay DasNoch keine Bewertungen
- CareerDokument35 SeitenCareerapi-178294569Noch keine Bewertungen
- 5 Conflict Management StylesDokument2 Seiten5 Conflict Management StylesVincent JNoch keine Bewertungen
- Promoting Self DeterminationDokument3 SeitenPromoting Self Determinationapi-295424948Noch keine Bewertungen
- Session 1 Principles of Child DevelopmentDokument27 SeitenSession 1 Principles of Child DevelopmentSalome LucasNoch keine Bewertungen
- Fears and FobiasDokument12 SeitenFears and FobiasmolesagNoch keine Bewertungen
- CSP 517 Mental Health ToolkitDokument53 SeitenCSP 517 Mental Health Toolkitapi-546386832Noch keine Bewertungen
- ADHD Workbook For Kids.Dokument154 SeitenADHD Workbook For Kids.saiyuktachhNoch keine Bewertungen
- Personality Disorders in AsiansDokument3 SeitenPersonality Disorders in AsiansIvee van GoghsiaNoch keine Bewertungen
- SLCS RDokument2 SeitenSLCS RdanieljohnarboledaNoch keine Bewertungen
- Soft Skills 35 F PR enDokument5 SeitenSoft Skills 35 F PR enapi-423847502Noch keine Bewertungen
- Understanding: Schizoaffective DisorderDokument24 SeitenUnderstanding: Schizoaffective DisorderGemma GarciaNoch keine Bewertungen
- Medical Report: Patient Name: Dob: ID: Clinic: Physician: Report DateDokument6 SeitenMedical Report: Patient Name: Dob: ID: Clinic: Physician: Report DateSudhansh KumarNoch keine Bewertungen
- Child Adolescent Perfectionism ScaleDokument1 SeiteChild Adolescent Perfectionism ScaleJeanaNoch keine Bewertungen
- Final EPQDokument19 SeitenFinal EPQtanishasen4Noch keine Bewertungen
- Violence and Suicide Assessment ScaleDokument8 SeitenViolence and Suicide Assessment ScaleAnonymous jYFfVGGNoch keine Bewertungen
- Aeps Assessment KaraDokument4 SeitenAeps Assessment Karaapi-206480101Noch keine Bewertungen
- ADHD in The Classroom: Effective Intervention Strategies: Theory Into PracticeDokument9 SeitenADHD in The Classroom: Effective Intervention Strategies: Theory Into PracticeGregorius Johan Putra KoentjanaNoch keine Bewertungen
- P427 - 14 - Structured Personality Tests - BWDokument6 SeitenP427 - 14 - Structured Personality Tests - BWHank RobinsonNoch keine Bewertungen
- PSI Policy Document - Guidelines For The Employment of Assistant PsychologistsDokument14 SeitenPSI Policy Document - Guidelines For The Employment of Assistant Psychologistsricosadie1Noch keine Bewertungen
- Body Language IDokument8 SeitenBody Language INuno Miguel FreitasNoch keine Bewertungen
- School Phobia PoerpointsDokument11 SeitenSchool Phobia PoerpointsInnoclazz AcademyNoch keine Bewertungen
- Neps Special Needs Resource PackDokument27 SeitenNeps Special Needs Resource PackMarta SilvaNoch keine Bewertungen
- Intro To Cognitive-Behavioral TherapyDokument49 SeitenIntro To Cognitive-Behavioral Therapywajiha yaminNoch keine Bewertungen
- Cognitive TherapyDokument18 SeitenCognitive TherapyHaysheryl Vallejo SalamancaNoch keine Bewertungen
- Understanding Asperger's Syndrome/Disorder - Parent GuideDokument6 SeitenUnderstanding Asperger's Syndrome/Disorder - Parent GuideCarol ToumehNoch keine Bewertungen
- Infant ReflexesDokument1 SeiteInfant ReflexesJohn Dela VegaNoch keine Bewertungen
- Nuggets of Wisdom Vol 1. Issue 2. Jan/Feb 2012Dokument4 SeitenNuggets of Wisdom Vol 1. Issue 2. Jan/Feb 2012InnerWisdomNoch keine Bewertungen
- PBL 3Dokument7 SeitenPBL 3UzmaNoch keine Bewertungen
- Take The Quiz: Please Note: This Test Will Only Be Scored Correctly If You Answer Each One of TheDokument4 SeitenTake The Quiz: Please Note: This Test Will Only Be Scored Correctly If You Answer Each One of TheAriane VidalNoch keine Bewertungen
- How-To-Cope-With-Hearing-Voices 2016Dokument22 SeitenHow-To-Cope-With-Hearing-Voices 2016api-247002951Noch keine Bewertungen
- Autism ModuleDokument4 SeitenAutism Moduleapi-2483017520% (1)
- ReaktorDokument46 SeitenReaktorSultan SetiawanNoch keine Bewertungen
- A Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)Dokument7 SeitenA Study On Customer Satisfaction Towards " Asian Paints" (With Reference To Hightech Paint Shopee, Adoni)RameshNoch keine Bewertungen
- PC 101 Life Skills: Gathering Agenda For Week 01Dokument3 SeitenPC 101 Life Skills: Gathering Agenda For Week 01juanNoch keine Bewertungen
- Development CLASSDokument33 SeitenDevelopment CLASSJulie JančíNoch keine Bewertungen
- EDPM Mark Scheme SBA Assignment 2 - 2017Dokument1 SeiteEDPM Mark Scheme SBA Assignment 2 - 2017ocamp200750% (2)
- Dokumen Penjajaran Kurikulum Bahasa Inggeris Tingkatan 2 KSSMDokument7 SeitenDokumen Penjajaran Kurikulum Bahasa Inggeris Tingkatan 2 KSSMQhairunisa HinsanNoch keine Bewertungen
- 2.use of Picture Dictionaries To Promote Functional Communication in Students With Deafness and Intellectual DisabilitiesDokument13 Seiten2.use of Picture Dictionaries To Promote Functional Communication in Students With Deafness and Intellectual DisabilitiesNor Siti RokiahNoch keine Bewertungen
- Writing The Précis: English For Academic and Professional PurposesDokument10 SeitenWriting The Précis: English For Academic and Professional PurposesDengDengNoch keine Bewertungen
- Ai NotesDokument76 SeitenAi NotesEPAH SIRENGONoch keine Bewertungen
- X & Y TheoryDokument16 SeitenX & Y Theoryanon_231950378100% (2)
- English 8: First Monthly ExaminationDokument2 SeitenEnglish 8: First Monthly ExaminationFloramie MorenoNoch keine Bewertungen
- MS401L16 Ready and Resilient Program SRDokument5 SeitenMS401L16 Ready and Resilient Program SRAlex LogvinovskyNoch keine Bewertungen
- COT 1 Plate Boundaries Science 10Dokument6 SeitenCOT 1 Plate Boundaries Science 10Christy Rose VelascoNoch keine Bewertungen
- FIRO Element BDokument19 SeitenFIRO Element Bnitin21822Noch keine Bewertungen
- Pe Assignment TopicsDokument2 SeitenPe Assignment Topicsapi-246838943Noch keine Bewertungen
- AEJ Special Edition December 2016 TESOL Indonesia Conference Volume 5Dokument218 SeitenAEJ Special Edition December 2016 TESOL Indonesia Conference Volume 5BimaNoch keine Bewertungen
- Bartle Elements of Integration and Lebesgue MeasureDokument20 SeitenBartle Elements of Integration and Lebesgue MeasureAlejandro FandiñoNoch keine Bewertungen
- Arjun Emf CVDokument2 SeitenArjun Emf CVArjun PrasadNoch keine Bewertungen
- Magic Mirror American English Teacher Ver2Dokument7 SeitenMagic Mirror American English Teacher Ver2COORDENAÇÃO FISK CAXIASNoch keine Bewertungen
- Mainframes ComputerDokument4 SeitenMainframes ComputerSarita SapaligaNoch keine Bewertungen
- Essay Writingg GuideDokument3 SeitenEssay Writingg GuideFlora Mae LacostalesNoch keine Bewertungen
- Behaviorally Anchored Rating ScalesDokument6 SeitenBehaviorally Anchored Rating Scalesmanoj2828Noch keine Bewertungen
- Spring Boot AnnotationsDokument12 SeitenSpring Boot AnnotationsMedNejjarNoch keine Bewertungen
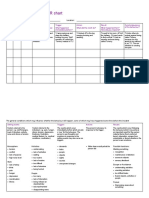
- Behaviour Recording Star Chart 1Dokument5 SeitenBehaviour Recording Star Chart 1api-629413258Noch keine Bewertungen
- Top 25 Test-Taking Tips, Suggestions & Strategies: WrongDokument5 SeitenTop 25 Test-Taking Tips, Suggestions & Strategies: WronglheanzNoch keine Bewertungen
- Friedman and Laurison - Excerpt From The Class CeilingDokument23 SeitenFriedman and Laurison - Excerpt From The Class CeilingRyuNoch keine Bewertungen
- Narrative-Descriptive Essay Marking SchemeDokument1 SeiteNarrative-Descriptive Essay Marking SchemeAlecsandra Andrei100% (1)
- Dhaval CVDokument2 SeitenDhaval CVPurva PrajapatiNoch keine Bewertungen
- Application of Soft Computing KCS056Dokument1 SeiteApplication of Soft Computing KCS056sahuritik314Noch keine Bewertungen
- Imeche Guidance Ieng Ceng V 14 MB WRDokument26 SeitenImeche Guidance Ieng Ceng V 14 MB WRRajiv ThambotheranNoch keine Bewertungen
- Metadata of The Chapter That Will Be Visualized Online: TantaleánDokument9 SeitenMetadata of The Chapter That Will Be Visualized Online: TantaleánHenry TantaleánNoch keine Bewertungen