Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- A Peritonsillar AbscessDokument10 SeitenA Peritonsillar AbscessAbdu RaheemNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- 3.17.08 Hyperparathyroidism SternDokument16 Seiten3.17.08 Hyperparathyroidism SternAbdu RaheemNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- HyponatremiaDokument42 SeitenHyponatremiaAbdu Raheem100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- HypomagnesimiaDokument16 SeitenHypomagnesimiaAbdu RaheemNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- HypocalcemiaDokument20 SeitenHypocalcemiaAbdu RaheemNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- ShockDokument115 SeitenShockAbdu RaheemNoch keine Bewertungen
- HyponatremiaDokument42 SeitenHyponatremiaAbdu Raheem100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- START Triage Training PresentationDokument85 SeitenSTART Triage Training PresentationAnita Amanda100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- PsychopharmacologyDokument77 SeitenPsychopharmacologychachaazkaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- S.5 BIO Reproduction in Animals NOTESDokument18 SeitenS.5 BIO Reproduction in Animals NOTESmusokelukia6Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Chapter 6 NeoplasiaDokument24 SeitenChapter 6 Neoplasiahenna patelNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Patent Ductus Arteriosus: by Dr. Hanan Zekri Khaled Lecturer of Pediatrics Pediatric CardiologyDokument36 SeitenPatent Ductus Arteriosus: by Dr. Hanan Zekri Khaled Lecturer of Pediatrics Pediatric CardiologyEira RajkumarNoch keine Bewertungen
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleDokument2 SeitenLaboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleumaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Bp503t Pcol Unit-VDokument46 SeitenBp503t Pcol Unit-VAakkkNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Air Layering Instructional SheetDokument6 SeitenAir Layering Instructional Sheetcandy_kb17Noch keine Bewertungen
- SRIVASTAVA & SINGH, 2008 - Brissid Echinoid Eupatagus From The Khuiala Formation, Jaisalmer District, Rajasthan, IndiaDokument6 SeitenSRIVASTAVA & SINGH, 2008 - Brissid Echinoid Eupatagus From The Khuiala Formation, Jaisalmer District, Rajasthan, Indiachindas4321Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Bioenergetics 1Dokument30 SeitenBioenergetics 1suni alditaNoch keine Bewertungen
- Prosthodontics Lec 4 PDFDokument11 SeitenProsthodontics Lec 4 PDFHassan QazaniNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hydra 1Dokument25 SeitenHydra 1Gowtham GupthaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Blg1502 Exam Prep Doc - Part 1&2Dokument18 SeitenBlg1502 Exam Prep Doc - Part 1&2Pasipanodya MuzendaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Kreisberg-Zakarin Et Al IPNS Antonie Van Leeuwenhoek 1999Dokument8 SeitenKreisberg-Zakarin Et Al IPNS Antonie Van Leeuwenhoek 1999ElNoch keine Bewertungen
- Heat ExhaustionDokument4 SeitenHeat Exhaustionapi-356829966Noch keine Bewertungen
- Agriculture& Horticulture Conference BrochureDokument6 SeitenAgriculture& Horticulture Conference BrochureAgriculture conferenceNoch keine Bewertungen
- Bandha Yoga. Tips and TechniquesDokument26 SeitenBandha Yoga. Tips and TechniquesTatjana Good100% (6)
- Neonatal PneumoniaDokument2 SeitenNeonatal PneumoniaJustin EduardoNoch keine Bewertungen
- Metabolism: Anabolism and CatabolismDokument4 SeitenMetabolism: Anabolism and CatabolismMedi OmicNoch keine Bewertungen
- Vedda+Blood+Sugar+Remedy+PDF+ +Book+Recipes+Free+Download+Michael+DempseyDokument20 SeitenVedda+Blood+Sugar+Remedy+PDF+ +Book+Recipes+Free+Download+Michael+DempseyBianca SmitheIncas AllenNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- BrodmannDokument2 SeitenBrodmannEdelleMojicaDafilmotoNoch keine Bewertungen
- Brooke Cybel TanateDokument5 SeitenBrooke Cybel TanateEbenezer Manguerra Diala Gube Jr.Noch keine Bewertungen
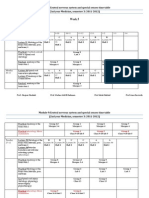
- Week 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Dokument17 SeitenWeek 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Hairul AnuarNoch keine Bewertungen
- Nano DentistryDokument6 SeitenNano DentistryanugrasNoch keine Bewertungen
- Survival at Sea For Mariners, Aviators PDFDokument178 SeitenSurvival at Sea For Mariners, Aviators PDFTrịnh Minh Khoa100% (1)
- AnatomyDokument8 SeitenAnatomyRobbie WoelkersNoch keine Bewertungen
- Choice of Enterostoma: Feeding Jejunostomy IleostomyDokument4 SeitenChoice of Enterostoma: Feeding Jejunostomy IleostomyFikranaya SalimNoch keine Bewertungen
- Mitochondrial Respiratory ComplexesDokument30 SeitenMitochondrial Respiratory ComplexesDouglas DíazNoch keine Bewertungen
- Aki 2018Dokument45 SeitenAki 2018NURUL ROMADHONNoch keine Bewertungen
- Strigo FungiDokument3 SeitenStrigo FungiMarc AmnésiaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)