Das könnte Ihnen auch gefallen
- Biological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentDokument63 SeitenBiological Warfare: Renaat A. A. M. Peleman, MD, PHD Dept Internal Med, Div Infect Dis University Hospital GhentAbdullah Al-RashedNoch keine Bewertungen
- 6-Laboratory Diagnosis For Infection DiseaseDokument42 Seiten6-Laboratory Diagnosis For Infection DiseaseTharshika MeanuNoch keine Bewertungen
- MD PPTDokument105 SeitenMD PPTtoxiczarrar.pubgNoch keine Bewertungen
- Preventive and Social MedicineDokument14 SeitenPreventive and Social MedicineSuresh GuduruNoch keine Bewertungen
- Review of Communicable DIsease NursingDokument252 SeitenReview of Communicable DIsease NursingRodelyn DariaNoch keine Bewertungen
- 13-Community Acquired PneumoniaDokument50 Seiten13-Community Acquired PneumoniaRubina MasihNoch keine Bewertungen
- Pulmonar y TuberculosisDokument35 SeitenPulmonar y TuberculosistuyalimonNoch keine Bewertungen
- Microbiology and Isolation Precaution, Dr. Agung, HISSI JatimDokument98 SeitenMicrobiology and Isolation Precaution, Dr. Agung, HISSI JatimEko Wahyu PradanaNoch keine Bewertungen
- Bioterror 120530Dokument58 SeitenBioterror 120530Marco R PaguiriganNoch keine Bewertungen
- Micr3011 NotesDokument3 SeitenMicr3011 NotesKatherine WangNoch keine Bewertungen
- Acute Pulmonary Infections: Zen Ahmad Medical Faculty, Sriwijaya UniversityDokument38 SeitenAcute Pulmonary Infections: Zen Ahmad Medical Faculty, Sriwijaya UniversitymayaNoch keine Bewertungen
- Lower Airway Dysfunctions: Margaret Xaira R. Mercado, RNDokument52 SeitenLower Airway Dysfunctions: Margaret Xaira R. Mercado, RNMargaret Xaira Rubio MercadoNoch keine Bewertungen
- PNEUMONIA - The Evil DiseaseDokument29 SeitenPNEUMONIA - The Evil Diseasesitesh009Noch keine Bewertungen
- Infection 2 1Dokument91 SeitenInfection 2 1saeedassaf97Noch keine Bewertungen
- Sumbul Parveen PneumoniaDokument27 SeitenSumbul Parveen Pneumoniaabhishekchoudhary81689Noch keine Bewertungen
- PneumoniaDokument53 SeitenPneumoniamrs raamNoch keine Bewertungen
- Tropmed - Lecture 4Dokument78 SeitenTropmed - Lecture 4VerarisnaNoch keine Bewertungen
- Pneumonia PDFDokument68 SeitenPneumonia PDFfatiniNoch keine Bewertungen
- PneumoniaDokument38 SeitenPneumoniaAzhar GhoriNoch keine Bewertungen
- Respiratory PandemicsDokument5 SeitenRespiratory PandemicsJiezl Abellano AfinidadNoch keine Bewertungen
- Arboviral Diseases and Dengue FinalDokument73 SeitenArboviral Diseases and Dengue FinalBinayaNoch keine Bewertungen
- TyphoidDokument67 SeitenTyphoidArnel L. SanicoNoch keine Bewertungen
- HAI's: DR Ridha Wahyutomo, SP - MK Clinical Microbiologist-Infection PreventionistDokument97 SeitenHAI's: DR Ridha Wahyutomo, SP - MK Clinical Microbiologist-Infection PreventionistRicky FerdiansyahNoch keine Bewertungen
- Corona VirusesDokument61 SeitenCorona VirusesNaing Lin SoeNoch keine Bewertungen
- PCAP Report - Mark ReyesDokument53 SeitenPCAP Report - Mark ReyesMark ReyesNoch keine Bewertungen
- Circulatory System: Nursing Care of Patient With Disease of TheDokument56 SeitenCirculatory System: Nursing Care of Patient With Disease of TheMada mada DaneNoch keine Bewertungen
- UntitledDokument6 SeitenUntitledRana zaatrehNoch keine Bewertungen
- DiphtheriaDokument22 SeitenDiphtheriaLovely Acabado TampocoNoch keine Bewertungen
- Tuberculosis AnakDokument26 SeitenTuberculosis AnakVaisnavi MuthoovalooNoch keine Bewertungen
- Anthrax and Ts PreventionDokument60 SeitenAnthrax and Ts PreventionZahid Qamar100% (1)
- Mol DiagnosticsDokument17 SeitenMol DiagnosticsjencyblessonNoch keine Bewertungen
- PneumoniaDokument27 SeitenPneumoniamameekasim75Noch keine Bewertungen
- Severe Acute Respiratory SyndromeDokument8 SeitenSevere Acute Respiratory SyndromeveralynnpNoch keine Bewertungen
- Anthrax: Didi CandradikusumaDokument40 SeitenAnthrax: Didi CandradikusumaFarrah Sayed100% (1)
- Non-Infectious Respiratory ProblemDokument66 SeitenNon-Infectious Respiratory ProblemSven OrdanzaNoch keine Bewertungen
- Nosocomial Infection. BPTDokument44 SeitenNosocomial Infection. BPTAanchal GuptaNoch keine Bewertungen
- Pulmonary Diseases - Dental ManagementDokument45 SeitenPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- Communicable DiseasesDokument123 SeitenCommunicable DiseasesAndrea Marie T. Artajo-BoheromNoch keine Bewertungen
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDokument28 Seiten3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaNoch keine Bewertungen
- Lower Respiratory Study SheetDokument13 SeitenLower Respiratory Study SheetJune Rhoades100% (2)
- Microbial Diseases of The Cardiovascular and Lymphatic SystemsDokument27 SeitenMicrobial Diseases of The Cardiovascular and Lymphatic SystemsAbhishek Isaac MathewNoch keine Bewertungen
- Upper Respıratory Tract InfectıonsDokument68 SeitenUpper Respıratory Tract InfectıonsMekdes ZewdeNoch keine Bewertungen
- Communicable Disease: Person To Person Microbial DiseasesDokument19 SeitenCommunicable Disease: Person To Person Microbial Diseasesnormina_balabagan9655Noch keine Bewertungen
- San Lazaro Question Bank SouthPark 2Dokument9 SeitenSan Lazaro Question Bank SouthPark 2Kenneth MiguelNoch keine Bewertungen
- Safe Handling, Packaging & Shipping of Infectious SubstancesDokument96 SeitenSafe Handling, Packaging & Shipping of Infectious SubstancesGeoffrey RufinNoch keine Bewertungen
- SWINE FINAL Update An Indain PrespectiveDokument92 SeitenSWINE FINAL Update An Indain PrespectiveperfectdocNoch keine Bewertungen
- PneumoniaDokument30 SeitenPneumoniaShakilaNoch keine Bewertungen
- Pediatric SepsisDokument57 SeitenPediatric SepsisSondang Herikson PanjaitanNoch keine Bewertungen
- Pneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptDokument30 SeitenPneumonia: Martianus P, S.Farm.,M.Farm - Klin.,AptmadewikewirantiNoch keine Bewertungen
- NOTES CD Lecture Generic 2022Dokument182 SeitenNOTES CD Lecture Generic 2022Meryville JacildoNoch keine Bewertungen
- Applied Therapeutic Ii FAR 454/3: Topic: MeningitisDokument14 SeitenApplied Therapeutic Ii FAR 454/3: Topic: MeningitisgentamicinNoch keine Bewertungen
- Tuberculosis: Divya MathewDokument42 SeitenTuberculosis: Divya MathewArun George0% (1)
- Anthrax: Humberto GuerraDokument60 SeitenAnthrax: Humberto GuerraLusia AdityaningtyasNoch keine Bewertungen
- Topic 2. Dyspnea. Complecated Pneumonia in Children. - ShortDokument69 SeitenTopic 2. Dyspnea. Complecated Pneumonia in Children. - ShortIbtissame BadadNoch keine Bewertungen
- Communicable DiseaseDokument98 SeitenCommunicable DiseasePeach BubbleNoch keine Bewertungen
- Leptospirosis Smt7Dokument34 SeitenLeptospirosis Smt7hendra_darmawan_4Noch keine Bewertungen
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDokument62 SeitenUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNoch keine Bewertungen
- PCAP Report - Mark ReyesDokument53 SeitenPCAP Report - Mark ReyesMark ReyesNoch keine Bewertungen
- PCAP Report - Mark ReyesDokument53 SeitenPCAP Report - Mark ReyesMark ReyesNoch keine Bewertungen
- Acute Renal Failure Chronic Renal FailureDokument48 SeitenAcute Renal Failure Chronic Renal Failurekimchi girlNoch keine Bewertungen
- Brand Name:: 1. Coronary Artery DiseaseDokument4 SeitenBrand Name:: 1. Coronary Artery Diseasekimchi girlNoch keine Bewertungen
- Osteogenesis Imperfecta Written ReportDokument16 SeitenOsteogenesis Imperfecta Written Reportkimchi girlNoch keine Bewertungen
- (MS) Stress Management PPT (Am)Dokument22 Seiten(MS) Stress Management PPT (Am)kimchi girl100% (1)
- Acute Coronary SyndromeDokument9 SeitenAcute Coronary Syndromekimchi girlNoch keine Bewertungen
- Criterion-Related ValidityDokument5 SeitenCriterion-Related Validitykimchi girlNoch keine Bewertungen
- Time Management: Prepared By: Lenila A. de Vera, RN, MPH, ManDokument11 SeitenTime Management: Prepared By: Lenila A. de Vera, RN, MPH, Mankimchi girlNoch keine Bewertungen
- A Client With Type 1 Diabetes: Nursing Care PlanDokument1 SeiteA Client With Type 1 Diabetes: Nursing Care Plankimchi girlNoch keine Bewertungen
- (NLM) Nursing Specialization PPT True (Am)Dokument120 Seiten(NLM) Nursing Specialization PPT True (Am)kimchi girlNoch keine Bewertungen
- Basic Nursing AssessmentDokument10 SeitenBasic Nursing AssessmentReza MioNoch keine Bewertungen
- DianeDokument3 SeitenDianekimchi girlNoch keine Bewertungen
- Newborn Screening Chapters 1 and 2 Partially 3iiiDokument31 SeitenNewborn Screening Chapters 1 and 2 Partially 3iiikimchi girlNoch keine Bewertungen
- Name Mechanism of Action Indication Contraindication Adverse/Side Effects Nursing Responsibilities Generic NameDokument1 SeiteName Mechanism of Action Indication Contraindication Adverse/Side Effects Nursing Responsibilities Generic Namekimchi girlNoch keine Bewertungen
- Criterion-Related ValidityDokument5 SeitenCriterion-Related Validitykimchi girlNoch keine Bewertungen
- Anesthesia Pocket GuideDokument16 SeitenAnesthesia Pocket Guidekimchi girl100% (2)
- Body LanguageDokument66 SeitenBody Languagekimchi girlNoch keine Bewertungen
- Eye Mucus Types: Identify The Mucus Coming From Your EyesDokument2 SeitenEye Mucus Types: Identify The Mucus Coming From Your Eyeskimchi girlNoch keine Bewertungen
- Bloom's TaxonomyDokument23 SeitenBloom's Taxonomykimchi girlNoch keine Bewertungen
- Presentation 1Dokument8 SeitenPresentation 1kimchi girlNoch keine Bewertungen
- NCPDokument5 SeitenNCPkimchi girl0% (1)
- Orientation PhaseDokument3 SeitenOrientation Phasekimchi girlNoch keine Bewertungen
- Assessment Nursing Diagnosis Background Knowledge Planning Nursing Intervention Rationale Evaluation Objective: Short-Term GoalDokument2 SeitenAssessment Nursing Diagnosis Background Knowledge Planning Nursing Intervention Rationale Evaluation Objective: Short-Term Goalkimchi girlNoch keine Bewertungen
- 13 ElectronicHealthRecordDokument48 Seiten13 ElectronicHealthRecordkimchi girl100% (1)
- NCPDokument5 SeitenNCPkimchi girl0% (1)
- Mr. Fida Hussain: Objective Academic QualificationDokument3 SeitenMr. Fida Hussain: Objective Academic QualificationBOBBY BEATSNoch keine Bewertungen
- AVN19941999Dokument96 SeitenAVN19941999Kate SquiresNoch keine Bewertungen
- The Determinants of Persistent Child Mortality Trend in UgandaDokument53 SeitenThe Determinants of Persistent Child Mortality Trend in UgandathinckollamNoch keine Bewertungen
- Upper Respiratory Tract Infection (Urti)Dokument2 SeitenUpper Respiratory Tract Infection (Urti)wen_pilNoch keine Bewertungen
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Dokument7 SeitenCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNoch keine Bewertungen
- 10exam 3rd PDokument4 Seiten10exam 3rd PLilet BadayosNoch keine Bewertungen
- EssayDokument61 SeitenEssayRevina AmaliaNoch keine Bewertungen
- Allergy: How Common Is Egg Allergy?Dokument6 SeitenAllergy: How Common Is Egg Allergy?Mohamed NabeilNoch keine Bewertungen
- SSCDokument310 SeitenSSCJoseNoch keine Bewertungen
- CHAPTER 1 - DraftDokument16 SeitenCHAPTER 1 - DraftARZELIE MARIE R. TOMBOCNoch keine Bewertungen
- Air Borne DiseasesDokument3 SeitenAir Borne DiseasesMuhammad Anwar GulNoch keine Bewertungen
- Noah's Ark Matchmaking Questionnaire 09Dokument3 SeitenNoah's Ark Matchmaking Questionnaire 09smgord2Noch keine Bewertungen
- Immunodot Torch Test 410346Dokument11 SeitenImmunodot Torch Test 410346Lucian MihuNoch keine Bewertungen
- Disease Questions 1 January 2021 No Mark SchemeDokument12 SeitenDisease Questions 1 January 2021 No Mark SchemeGus PneumaticosNoch keine Bewertungen
- Australia Visa PDFDokument6 SeitenAustralia Visa PDFminjiew50% (2)
- Scope of ImmunologyDokument6 SeitenScope of ImmunologySulove Koirala100% (3)
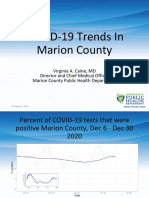
- Marion County Public Health Update 01.07.21Dokument15 SeitenMarion County Public Health Update 01.07.21Last DayNoch keine Bewertungen
- Maklumat Vaksinasi: Vaccination DetailsDokument2 SeitenMaklumat Vaksinasi: Vaccination DetailsImtiaz EmpireNoch keine Bewertungen
- CHAPTER 7 Pricing and DrugsDokument34 SeitenCHAPTER 7 Pricing and DrugsS.Srinivasan ('Chinu'); Renu Khanna100% (1)
- USP 51. Antimicrobial Effectiveness TestingDokument4 SeitenUSP 51. Antimicrobial Effectiveness TestingAgeng Wahyu Patrianita100% (1)
- Avian Encephalomyelitis (AE)Dokument22 SeitenAvian Encephalomyelitis (AE)Dr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (1)
- Prelim Exam NCM 103Dokument10 SeitenPrelim Exam NCM 103Zhyraine Iraj D. CaluzaNoch keine Bewertungen
- PandemicsDokument41 SeitenPandemicsapi-3706215Noch keine Bewertungen
- Borang Warrant To Act Ibubapa-Anak2Dokument3 SeitenBorang Warrant To Act Ibubapa-Anak2lawrencekailNoch keine Bewertungen
- Science G 5 Model Paper Part ADokument4 SeitenScience G 5 Model Paper Part Aapi-251341286Noch keine Bewertungen
- EYE Emergency Manual An Illustrated Guide: Second EditionDokument56 SeitenEYE Emergency Manual An Illustrated Guide: Second Editionmanleyj5305Noch keine Bewertungen
- Communicable DiseasesDokument164 SeitenCommunicable DiseasesJasmin Jacob33% (3)
- Respiratory Problems of Poultry & Application of Vaccines: Dr. Mohammad AkramDokument92 SeitenRespiratory Problems of Poultry & Application of Vaccines: Dr. Mohammad Akramthanh ba matNoch keine Bewertungen
- MEASLES PresentationDokument29 SeitenMEASLES PresentationMobin Ur Rehman Khan100% (3)
- Cefadroxil: Antibiotic ClassDokument2 SeitenCefadroxil: Antibiotic ClassTariNoch keine Bewertungen
- You Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherVon EverandYou Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherNoch keine Bewertungen
- The House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedVon EverandThe House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedBewertung: 4.5 von 5 Sternen4.5/5 (5)
- The Importance of Being Earnest: Classic Tales EditionVon EverandThe Importance of Being Earnest: Classic Tales EditionBewertung: 4.5 von 5 Sternen4.5/5 (44)
- The Inimitable Jeeves [Classic Tales Edition]Von EverandThe Inimitable Jeeves [Classic Tales Edition]Bewertung: 5 von 5 Sternen5/5 (3)
- The Comedians in Cars Getting Coffee BookVon EverandThe Comedians in Cars Getting Coffee BookBewertung: 4.5 von 5 Sternen4.5/5 (8)
- The Book of Bad:: Stuff You Should Know Unless You’re a PussyVon EverandThe Book of Bad:: Stuff You Should Know Unless You’re a PussyBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Sex, Drugs, and Cocoa Puffs: A Low Culture ManifestoVon EverandSex, Drugs, and Cocoa Puffs: A Low Culture ManifestoBewertung: 3.5 von 5 Sternen3.5/5 (1428)
- The Most Forbidden Knowledge: 151 Things NO ONE Should Know How to DoVon EverandThe Most Forbidden Knowledge: 151 Things NO ONE Should Know How to DoBewertung: 4.5 von 5 Sternen4.5/5 (6)
- Take My Advice: Letters to the Next Generation from People Who Know a Thing or TwoVon EverandTake My Advice: Letters to the Next Generation from People Who Know a Thing or TwoJames L. HarmonBewertung: 4 von 5 Sternen4/5 (5)
- Welcome to the United States of Anxiety: Observations from a Reforming NeuroticVon EverandWelcome to the United States of Anxiety: Observations from a Reforming NeuroticBewertung: 3.5 von 5 Sternen3.5/5 (10)
- The Smartest Book in the World: A Lexicon of Literacy, A Rancorous Reportage, A Concise Curriculum of CoolVon EverandThe Smartest Book in the World: A Lexicon of Literacy, A Rancorous Reportage, A Concise Curriculum of CoolBewertung: 4 von 5 Sternen4/5 (14)