Das könnte Ihnen auch gefallen
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- UNIT - 10 Infection Control: MeasuresDokument27 SeitenUNIT - 10 Infection Control: MeasuresReeycha ShresthaNoch keine Bewertungen
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesVon EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNoch keine Bewertungen
- Health Problems MyselfDokument54 SeitenHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Respiratory System DisordersDokument9 SeitenRespiratory System Disordersasop06Noch keine Bewertungen
- TB MeningitisDokument17 SeitenTB MeningitisSylvan LaminaNoch keine Bewertungen
- Overview of India's Revised National Tuberculosis Control ProgrammeDokument65 SeitenOverview of India's Revised National Tuberculosis Control Programmecatalyst1986100% (1)
- Health Promotion (Eng)Dokument25 SeitenHealth Promotion (Eng)JaneLorensNoch keine Bewertungen
- Introduction To Community Health NursingDokument23 SeitenIntroduction To Community Health NursingAlmasNoch keine Bewertungen
- NHP 2Dokument42 SeitenNHP 2A J FathimaNoch keine Bewertungen
- National Health Programmes For Children in IndiaDokument79 SeitenNational Health Programmes For Children in IndiashahnazNoch keine Bewertungen
- TyphoidDokument10 SeitenTyphoidpeterjongNoch keine Bewertungen
- Promoting Safety in Healthcare EnvDokument13 SeitenPromoting Safety in Healthcare EnvnamNoch keine Bewertungen
- Vijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyDokument3 SeitenVijaya College of Nursing: Course Subject Unit Bio-Psycho Social PathophysiologyReshma Rinu50% (2)
- Sterilization and DisinfectionDokument68 SeitenSterilization and DisinfectionMohammed Qasim Al-WataryNoch keine Bewertungen
- HypothermiaDokument5 SeitenHypothermiaMRS CHAKRAPANINoch keine Bewertungen
- Good Touch Bad Touch - A Student's Perspective On Child SafetyDokument2 SeitenGood Touch Bad Touch - A Student's Perspective On Child SafetyAbhijeet Rajpurohit100% (1)
- Nature of InfectionDokument10 SeitenNature of InfectionHussain FaqirjeeNoch keine Bewertungen
- Disinfection and SterilisationDokument36 SeitenDisinfection and SterilisationvaidyamNoch keine Bewertungen
- What Is A Cross Infection?Dokument5 SeitenWhat Is A Cross Infection?nandyta febryani100% (2)
- Epidemiology of Non-Communicable DiseasesDokument16 SeitenEpidemiology of Non-Communicable DiseasesAparna AbyNoch keine Bewertungen
- Nosocomial InfectionDokument13 SeitenNosocomial InfectionwabalyNoch keine Bewertungen
- Pneumonia: Diagnosis, Treatment and ManagementDokument30 SeitenPneumonia: Diagnosis, Treatment and ManagementShakilaNoch keine Bewertungen
- Esophageal CancerDokument25 SeitenEsophageal CancerK poojithaNoch keine Bewertungen
- Guidance & Counseling": Rajesh Kumar LecturerDokument19 SeitenGuidance & Counseling": Rajesh Kumar LecturerLove DhaliwalNoch keine Bewertungen
- GERIATRIC CONSIDERATIONS IN NURSINGDokument70 SeitenGERIATRIC CONSIDERATIONS IN NURSINGsanthiyasandy100% (1)
- Food HygieneDokument31 SeitenFood Hygienehemihema100% (1)
- Epidemiology AssignmentDokument12 SeitenEpidemiology AssignmentSagar ParajuliNoch keine Bewertungen
- Hepatic Encephalopathy: Causes, Tests, and Treatment OptionsVon EverandHepatic Encephalopathy: Causes, Tests, and Treatment OptionsBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Nursing Management of Patients Occupational and Industrial DisordersDokument11 SeitenNursing Management of Patients Occupational and Industrial DisordersNandini VermaNoch keine Bewertungen
- AMOEBIASISDokument31 SeitenAMOEBIASISpriyagerard100% (1)
- Nosocomial InfectionDokument16 SeitenNosocomial Infectionmarissa ulkhairNoch keine Bewertungen
- RNTCPDokument32 SeitenRNTCPSuvendu Sekhar PandaNoch keine Bewertungen
- Hepatitis in ChildrenDokument2 SeitenHepatitis in ChildrenShilpi SinghNoch keine Bewertungen
- Bronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)Dokument29 SeitenBronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)HimanshiNoch keine Bewertungen
- TyphusDokument21 SeitenTyphusJ J MEDIANoch keine Bewertungen
- Kod Kursus-JIB 533 Nama Kursus: Public Health Nama Pengurus Kursus Dr. Rohayu HamiDokument55 SeitenKod Kursus-JIB 533 Nama Kursus: Public Health Nama Pengurus Kursus Dr. Rohayu HamiNurfaizuraNoch keine Bewertungen
- Hookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilDokument5 SeitenHookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilBrix Valdriz100% (1)
- Disposable Delivery KitDokument13 SeitenDisposable Delivery Kitapi-3823785100% (1)
- Epidemilogy Measurment MethodsDokument100 SeitenEpidemilogy Measurment MethodsKailash NagarNoch keine Bewertungen
- Chicken Pox and Herpes ZosterfinalDokument31 SeitenChicken Pox and Herpes ZosterfinalBinayaNoch keine Bewertungen
- MeningitisDokument12 SeitenMeningitisFaith Vaughn100% (2)
- Essential Components of Palliative CareDokument13 SeitenEssential Components of Palliative Careleian28100% (1)
- Food Production & AdulterationDokument23 SeitenFood Production & Adulterationvinoth100% (1)
- Congenital AbnormalitiesDokument45 SeitenCongenital AbnormalitiesSaad AbdullahNoch keine Bewertungen
- Standard Precautions PolicyDokument8 SeitenStandard Precautions PolicyMasrov TukirovNoch keine Bewertungen
- MumpsDokument11 SeitenMumpscasandra moranteNoch keine Bewertungen
- Safemotherhood 130212085105 Phpapp01Dokument32 SeitenSafemotherhood 130212085105 Phpapp01daniel laoatenNoch keine Bewertungen
- 8A Nosocomial InfectionDokument15 Seiten8A Nosocomial InfectionSuminaShrestha100% (1)
- National Health Programs for Cardiovascular and Respiratory ConditionsDokument7 SeitenNational Health Programs for Cardiovascular and Respiratory ConditionsJyoti singhNoch keine Bewertungen
- SodaPDF-converted-lesson Plan of Cervical Cancer For ResearchDokument54 SeitenSodaPDF-converted-lesson Plan of Cervical Cancer For ResearchPatel KrimaNoch keine Bewertungen
- Universal PrecautionDokument10 SeitenUniversal PrecautionParth VasaveNoch keine Bewertungen
- Adrenal TumorsDokument21 SeitenAdrenal TumorsAlice sylviya Samuel100% (1)
- Reproductive Tract InfectionDokument48 SeitenReproductive Tract InfectionSampriti Roy100% (1)
- SummaryDokument4 SeitenSummaryDyam MitchNoch keine Bewertungen
- Measures of Health PromotionDokument68 SeitenMeasures of Health PromotionSamjhana Neupane100% (1)
- npcdcs-22 04 2020Dokument38 Seitennpcdcs-22 04 2020Neethu VincentNoch keine Bewertungen
- CVP MonitoringDokument24 SeitenCVP MonitoringChoji Heiwajima100% (1)
- Hiv and Aids in ChildrenDokument36 SeitenHiv and Aids in ChildrenKazau FwalangaNoch keine Bewertungen
- Robbins Chapter 1 Cell As A Unit of Health and DiseaseDokument46 SeitenRobbins Chapter 1 Cell As A Unit of Health and DiseaseDr. Ashish Jawarkar0% (1)
- External Examination at AutopsyDokument87 SeitenExternal Examination at AutopsyDr. Ashish JawarkarNoch keine Bewertungen
- Anti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDokument41 SeitenAnti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDr. Ashish JawarkarNoch keine Bewertungen
- Systemic Microbiology: BacteriologyDokument42 SeitenSystemic Microbiology: BacteriologyDr. Ashish JawarkarNoch keine Bewertungen
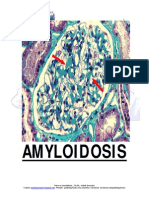
- AmyloidosisDokument26 SeitenAmyloidosisDr. Ashish JawarkarNoch keine Bewertungen
- Semen Analysis (WHO 2010)Dokument14 SeitenSemen Analysis (WHO 2010)Dr. Ashish Jawarkar100% (1)
- Control of Aerosol Transmitted DiseasesDokument45 SeitenControl of Aerosol Transmitted DiseasesDr. Ashish JawarkarNoch keine Bewertungen
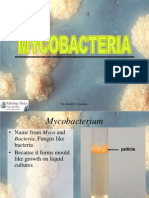
- MycobacteriaDokument62 SeitenMycobacteriaDr. Ashish JawarkarNoch keine Bewertungen
- StreptococciDokument91 SeitenStreptococciDr. Ashish JawarkarNoch keine Bewertungen
- Control of Microbial Growth: Dr. Ashish Jawarkar Pathologist Parul Sevashram HospitalDokument38 SeitenControl of Microbial Growth: Dr. Ashish Jawarkar Pathologist Parul Sevashram HospitalDr. Ashish JawarkarNoch keine Bewertungen
- Needle Sticks Sharps Injuries: FactsDokument31 SeitenNeedle Sticks Sharps Injuries: FactsDr. Ashish Jawarkar67% (3)
- Blood and Its ComponentsDokument72 SeitenBlood and Its ComponentsDr. Ashish JawarkarNoch keine Bewertungen
- Biomedical Waste ManagementDokument57 SeitenBiomedical Waste ManagementDr. Ashish JawarkarNoch keine Bewertungen
- Sickle Cell AnemiaDokument13 SeitenSickle Cell AnemiaDr. Ashish JawarkarNoch keine Bewertungen
- Laboratory Approach To AnemiasDokument23 SeitenLaboratory Approach To AnemiasDr. Ashish JawarkarNoch keine Bewertungen
- Laboratory Approach To Bleeding DisordersDokument33 SeitenLaboratory Approach To Bleeding DisordersDr. Ashish JawarkarNoch keine Bewertungen
- Thyroid Function TestsDokument21 SeitenThyroid Function TestsDr. Ashish JawarkarNoch keine Bewertungen
- Sputum ExaminationDokument9 SeitenSputum ExaminationDr. Ashish JawarkarNoch keine Bewertungen
- Infections and ImmunityDokument35 SeitenInfections and ImmunityDr. Ashish JawarkarNoch keine Bewertungen
- Renal Function TestsDokument26 SeitenRenal Function TestsDr. Ashish Jawarkar100% (1)
- Microbiology Quiz 2Dokument52 SeitenMicrobiology Quiz 2Dr. Ashish JawarkarNoch keine Bewertungen
- Liver Function TestsDokument28 SeitenLiver Function TestsDr. Ashish Jawarkar100% (2)
- Microscopy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDokument21 SeitenMicroscopy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDr. Ashish JawarkarNoch keine Bewertungen
- Pregnancy TestsDokument9 SeitenPregnancy TestsDr. Ashish JawarkarNoch keine Bewertungen
- Microbiology Quiz 1Dokument47 SeitenMicrobiology Quiz 1Dr. Ashish JawarkarNoch keine Bewertungen
- Bacteria: Morphology and ClassificationDokument44 SeitenBacteria: Morphology and ClassificationDr. Ashish JawarkarNoch keine Bewertungen
- Sterilization and DisinfectionDokument68 SeitenSterilization and DisinfectionDr. Ashish Jawarkar100% (1)
- Basics of Microscopy and StainingDokument29 SeitenBasics of Microscopy and StainingDr. Ashish JawarkarNoch keine Bewertungen
- Culture Methods and Culture MediaDokument48 SeitenCulture Methods and Culture MediaDr. Ashish JawarkarNoch keine Bewertungen
- 01 - 01 - SK10 - JXNipponDokument1 Seite01 - 01 - SK10 - JXNipponredevils86Noch keine Bewertungen
- Material Handling EquipmentsDokument12 SeitenMaterial Handling EquipmentsRahul SheelavantarNoch keine Bewertungen
- Merit of RatingDokument1 SeiteMerit of RatingRaidasNoch keine Bewertungen
- Endocrown Review 1Dokument9 SeitenEndocrown Review 1Anjali SatsangiNoch keine Bewertungen
- Carpentry Shop: Building, Doors, Windows, Trusses, WorkbenchesDokument105 SeitenCarpentry Shop: Building, Doors, Windows, Trusses, WorkbenchesVinod KumarNoch keine Bewertungen
- 10059-DC-K-01-A Design BasisDokument34 Seiten10059-DC-K-01-A Design BasisAnonymous RvIgDUNoch keine Bewertungen
- Cellular Basis of HeredityDokument12 SeitenCellular Basis of HeredityLadyvirdi CarbonellNoch keine Bewertungen
- Business Startup Practical Plan PDFDokument70 SeitenBusiness Startup Practical Plan PDFShaji Viswanathan. Mcom, MBA (U.K)Noch keine Bewertungen
- Nursing Care PlansDokument10 SeitenNursing Care PlansGracie S. Vergara100% (1)
- Maximizing Oredrive Development at Khoemacau MineDokument54 SeitenMaximizing Oredrive Development at Khoemacau MineModisa SibungaNoch keine Bewertungen
- Emission of Volatile Organic Compounds (Vocs) From Dispersion and Cementitious Waterproofing ProductsDokument16 SeitenEmission of Volatile Organic Compounds (Vocs) From Dispersion and Cementitious Waterproofing ProductsKrishna KusumaNoch keine Bewertungen
- ItilDokument11 SeitenItilNarendar P100% (2)
- 2 English Course BDokument8 Seiten2 English Course BAnjana27Noch keine Bewertungen
- Bio-Tank Guidelines for Indian RailwayDokument51 SeitenBio-Tank Guidelines for Indian Railwayravi100% (2)
- Synthesis, Experimental and Theoretical Characterizations of A NewDokument7 SeitenSynthesis, Experimental and Theoretical Characterizations of A NewWail MadridNoch keine Bewertungen
- Case Studies On Industrial Accidents - 2Dokument84 SeitenCase Studies On Industrial Accidents - 2Parth N Bhatt100% (2)
- HVDC BasicDokument36 SeitenHVDC BasicAshok KumarNoch keine Bewertungen
- Rudraksha - Scientific FactsDokument20 SeitenRudraksha - Scientific FactsAkash Agarwal100% (3)
- 2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and ChildDokument3 Seiten2.1. Pharmacological Therapeutics. 2.2. Basic Cardiac Life Support (BCLS) and Advanced Cardiac Life Support (ACLS) in Neonates and Childclint xavier odangoNoch keine Bewertungen
- Dr. Namrata Misra Head of Bioinnovations at KIIT UniversityDokument1 SeiteDr. Namrata Misra Head of Bioinnovations at KIIT Universitymanisha maniNoch keine Bewertungen
- PHAR342 Answer Key 5Dokument4 SeitenPHAR342 Answer Key 5hanif pangestuNoch keine Bewertungen
- AAR Maintenance 001Dokument3 SeitenAAR Maintenance 001prakash reddyNoch keine Bewertungen
- Block 1 Board Review - Lecture NotesDokument127 SeitenBlock 1 Board Review - Lecture NotesCece RereNoch keine Bewertungen
- Switzerland: Food and CultureDokument18 SeitenSwitzerland: Food and CultureAaron CoutinhoNoch keine Bewertungen
- Space Analysis in Orthodontic: University of GlasgowDokument16 SeitenSpace Analysis in Orthodontic: University of GlasgowNizam Muhamad100% (1)
- Hinduism Today April May June 2015Dokument43 SeitenHinduism Today April May June 2015jpmahadevNoch keine Bewertungen
- Exercise 4 Summary - KEY PDFDokument3 SeitenExercise 4 Summary - KEY PDFFrida Olea100% (1)
- Executive Order 000Dokument2 SeitenExecutive Order 000Randell ManjarresNoch keine Bewertungen
- EEDMATH1 - Teaching Mathematics in The Primary Grades Beed 2E Learning Activity PlanDokument3 SeitenEEDMATH1 - Teaching Mathematics in The Primary Grades Beed 2E Learning Activity PlanBELJUNE MARK GALANANNoch keine Bewertungen
- FINALS REVIEWER ENVI ENGG Topic 1Dokument8 SeitenFINALS REVIEWER ENVI ENGG Topic 1As ReNoch keine Bewertungen