Das könnte Ihnen auch gefallen
- Jesus Hold My Hand EbDokument2 SeitenJesus Hold My Hand EbGregg100% (3)
- Bone Tumor - Dr. Andri R. Winoto, SpOT (K)Dokument19 SeitenBone Tumor - Dr. Andri R. Winoto, SpOT (K)Aramanda DianNoch keine Bewertungen
- Musculoskeletal Tumor ManagementDokument16 SeitenMusculoskeletal Tumor ManagementRonald TejoprayitnoNoch keine Bewertungen
- Orthopedics 5 Year SolveDokument5 SeitenOrthopedics 5 Year SolveChowdhury Mohammed Tawhid TasneefNoch keine Bewertungen
- Chronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDokument31 SeitenChronic Osteomyelitis: Dr. F. Abdul Khader Professor & HOD Department of Orthopaedics SSSMC & RiDr. F. Abdul KhaderNoch keine Bewertungen
- Musculoskeletal TumorDokument89 SeitenMusculoskeletal TumorHayaNoch keine Bewertungen
- Chronic OsteomyelitisDokument29 SeitenChronic OsteomyelitisAbdul BasitNoch keine Bewertungen
- The Most Common Primary Malignant Tumor of The BoneDokument28 SeitenThe Most Common Primary Malignant Tumor of The BoneandhitaNoch keine Bewertungen
- Tumor Tulang Jinak: Anisah Mahmudah C014172125Dokument18 SeitenTumor Tulang Jinak: Anisah Mahmudah C014172125Williamtatokieesz Tembokrumahampebenjol-benjolNoch keine Bewertungen
- 6.musculoskeletal TumorsDokument110 Seiten6.musculoskeletal Tumorslina jamalNoch keine Bewertungen
- Temporomandibular Joint DiseaseDokument84 SeitenTemporomandibular Joint Diseaseapi-19916399Noch keine Bewertungen
- Neoplasms of The Musculoskeletal TissuesDokument21 SeitenNeoplasms of The Musculoskeletal Tissuesi dewa wisnu putraNoch keine Bewertungen
- Bony Ankylosis Mimicking Benign ChondromaDokument4 SeitenBony Ankylosis Mimicking Benign ChondromaAnumita DekaNoch keine Bewertungen
- Bone and Joint Neoplasm or TumorDokument49 SeitenBone and Joint Neoplasm or Tumorendah rahmadaniNoch keine Bewertungen
- 1 s2.0 S2049080122008718 MainDokument4 Seiten1 s2.0 S2049080122008718 MainFarizka Dwinda HidayatNoch keine Bewertungen
- Two Cases of Masticator Space Abscess Initially Diagnosed As Temporomandibular Joint DisorderDokument6 SeitenTwo Cases of Masticator Space Abscess Initially Diagnosed As Temporomandibular Joint DisorderdokteryopiNoch keine Bewertungen
- Dr. Ronald V. Munthe Spot SMF Bedah Rs UkiDokument50 SeitenDr. Ronald V. Munthe Spot SMF Bedah Rs UkiOdilia Maria RahalusNoch keine Bewertungen
- Jaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & IpgmerDokument28 SeitenJaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & Ipgmerdevinchi09Noch keine Bewertungen
- A Case Report of Hydatid Disease in Long BoneDokument4 SeitenA Case Report of Hydatid Disease in Long BoneVarun ArunagiriNoch keine Bewertungen
- Low-Grade Osteosarcoma of The MandibleDokument5 SeitenLow-Grade Osteosarcoma of The MandibleGalih AryyagunawanNoch keine Bewertungen
- Xray of Bones in OsteomyelitisDokument35 SeitenXray of Bones in OsteomyelitisBukola AjokeNoch keine Bewertungen
- Mastoid Osteoma of Temporal Bone - A Rare Case ReportDokument2 SeitenMastoid Osteoma of Temporal Bone - A Rare Case Reportreza salzabellaNoch keine Bewertungen
- Anatomy of The Upper and Lower Extremities Neoplasms of MusculosDokument93 SeitenAnatomy of The Upper and Lower Extremities Neoplasms of MusculosraihanekapNoch keine Bewertungen
- 'Osteomyelitis'6 4Dokument8 Seiten'Osteomyelitis'6 4b5mkn9h6pkNoch keine Bewertungen
- Radiologic Imaging of MuskuloskeletalDokument42 SeitenRadiologic Imaging of MuskuloskeletalfennyhasanahNoch keine Bewertungen
- EGZCR3Dokument4 SeitenEGZCR3Diyah Ayu Nur SantiNoch keine Bewertungen
- Badel 289 292Dokument4 SeitenBadel 289 292Catalina Soler LioiNoch keine Bewertungen
- Radio Logical Assessment of OA FinalDokument60 SeitenRadio Logical Assessment of OA FinaltarikeopsNoch keine Bewertungen
- Malignant Bone TumoursDokument38 SeitenMalignant Bone Tumoursgdudex118811Noch keine Bewertungen
- Osteomyelitis of The Jaws - 52Dokument52 SeitenOsteomyelitis of The Jaws - 52hazeemmegahedNoch keine Bewertungen
- JCM 11 00166 With CoverDokument29 SeitenJCM 11 00166 With CoverBruno MañonNoch keine Bewertungen
- Osteochondroma of The Coronoid Process of The MandibleDokument4 SeitenOsteochondroma of The Coronoid Process of The MandiblegtawidhiNoch keine Bewertungen
- GCG Palate PDC 15 - 4 - 135Dokument5 SeitenGCG Palate PDC 15 - 4 - 135Yiu Kai WongNoch keine Bewertungen
- Bone tm3Dokument57 SeitenBone tm3ZakiyahulfahdwNoch keine Bewertungen
- IJRID28Dokument10 SeitenIJRID28Saurabh SatheNoch keine Bewertungen
- Department of Orthopaedics: ModeratorsDokument31 SeitenDepartment of Orthopaedics: ModeratorschinmayghaisasNoch keine Bewertungen
- The Variable Imaging Appearance of OsteosarcomaDokument5 SeitenThe Variable Imaging Appearance of OsteosarcomaHenry LaksmanaNoch keine Bewertungen
- Giant Cell Tumor of Distal End of Femur With Pathological Fracture Treated by Resection and Megaprosthesis A Case ReportDokument5 SeitenGiant Cell Tumor of Distal End of Femur With Pathological Fracture Treated by Resection and Megaprosthesis A Case ReportInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Cranium 3Dokument26 SeitenCranium 3giant nitaNoch keine Bewertungen
- Bone and Joint TumoursDokument49 SeitenBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Giant Cell TumourDokument61 SeitenGiant Cell Tumourvictormoirangthem100% (1)
- Idiopathic Condylar ResorptionbDokument12 SeitenIdiopathic Condylar ResorptionbBelizNoch keine Bewertungen
- Osteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityDokument48 SeitenOsteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityPercy Linares MorilloNoch keine Bewertungen
- 2021 Publication Case Report - Frontal MucoceleDokument3 Seiten2021 Publication Case Report - Frontal MucoceleMade RusmanaNoch keine Bewertungen
- Myeloma MultipleDokument7 SeitenMyeloma MultipleCriissthiiann HernnandezNoch keine Bewertungen
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Dokument225 SeitenBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNoch keine Bewertungen
- Angiomyolipoma of The Hard Palate: Clinical ReportDokument2 SeitenAngiomyolipoma of The Hard Palate: Clinical ReportKezia Rachellea MustakimNoch keine Bewertungen
- Diagnosis and Management of Osteomyelitis: Gunawan, B SetiyohadiDokument5 SeitenDiagnosis and Management of Osteomyelitis: Gunawan, B SetiyohadiAndre PhanNoch keine Bewertungen
- Wijaya Johanes Chendra, DR., SP - OTDokument41 SeitenWijaya Johanes Chendra, DR., SP - OTRiqqah USNoch keine Bewertungen
- Tumours: Apley 9th Ed p.187-223Dokument66 SeitenTumours: Apley 9th Ed p.187-223Helmi IsmunandarNoch keine Bewertungen
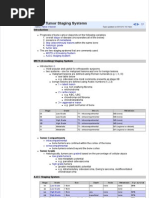
- Bone Tumour Staging - PathologyDokument2 SeitenBone Tumour Staging - Pathologyo7113Noch keine Bewertungen
- Management of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportDokument5 SeitenManagement of Non-Metastatic Pelvic Bone Giant Cell Tumour by Resection, Extended Curettage and Reconstruction With Autograft and Allograft - A Case ReportInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- GCT PDFDokument6 SeitenGCT PDFsandeep nemaNoch keine Bewertungen
- Lippincott Pathology QuestionsDokument10 SeitenLippincott Pathology Questionsابواحمد المجاهدNoch keine Bewertungen
- Bone TumorsDokument6 SeitenBone Tumorsa179360Noch keine Bewertungen
- Magnetic Resonance Imaging of Diabetic Foot Complications: RticleDokument12 SeitenMagnetic Resonance Imaging of Diabetic Foot Complications: RticlenessimNoch keine Bewertungen
- Infected Non Union1Dokument41 SeitenInfected Non Union1SyarifNoch keine Bewertungen
- Research ArticleDokument9 SeitenResearch ArticleAni LabibahNoch keine Bewertungen
- Pathology of Bone and Soft Tissue-LectureDokument52 SeitenPathology of Bone and Soft Tissue-Lecturejohnwickshopping79Noch keine Bewertungen
- Okc PDFDokument6 SeitenOkc PDFanggiNoch keine Bewertungen
- Pembahasan TBL Kardiologi IDokument153 SeitenPembahasan TBL Kardiologi IRizqon Yassir KuswondoNoch keine Bewertungen
- Jurnal Reading HFDokument34 SeitenJurnal Reading HFRizqon Yassir KuswondoNoch keine Bewertungen
- (Journal Reading) A Randomized Trial of Adenotonsillectomy For Childhood Sleep ApneaDokument27 Seiten(Journal Reading) A Randomized Trial of Adenotonsillectomy For Childhood Sleep ApneaRizqon Yassir KuswondoNoch keine Bewertungen
- Adrian Hardec Nasdal Modul 6 LBM 2Dokument9 SeitenAdrian Hardec Nasdal Modul 6 LBM 2Rizqon Yassir KuswondoNoch keine Bewertungen
- Fisiologi Hati Dan Kandung EmpeduDokument37 SeitenFisiologi Hati Dan Kandung EmpeduRizqon Yassir KuswondoNoch keine Bewertungen
- BUS 301 - Hospitality Industry Vietnam - Nguyễn Thị Thanh Thuý - 1632300205Dokument55 SeitenBUS 301 - Hospitality Industry Vietnam - Nguyễn Thị Thanh Thuý - 1632300205Nguyễn Thị Thanh ThúyNoch keine Bewertungen
- Chapter 14ADokument52 SeitenChapter 14Arajan35Noch keine Bewertungen
- Sugar Industries of PakistanDokument19 SeitenSugar Industries of Pakistanhelperforeu50% (2)
- Pudlo CWP TDS 2Dokument4 SeitenPudlo CWP TDS 2azharNoch keine Bewertungen
- Daftar PustakaDokument6 SeitenDaftar PustakaSeptian UtamaNoch keine Bewertungen
- Project CharterDokument10 SeitenProject CharterAdnan AhmedNoch keine Bewertungen
- RPS Manajemen Keuangan IIDokument2 SeitenRPS Manajemen Keuangan IIaulia endiniNoch keine Bewertungen
- Laws and Policies of Fertilizers SectorDokument12 SeitenLaws and Policies of Fertilizers Sectorqry01327Noch keine Bewertungen
- Industrial Cpmplus Enterprise Connectivity Collaborative Production ManagementDokument8 SeitenIndustrial Cpmplus Enterprise Connectivity Collaborative Production ManagementEng Ahmad Bk AlbakheetNoch keine Bewertungen
- Surge Protectionfor ACMachineryDokument8 SeitenSurge Protectionfor ACMachineryvyroreiNoch keine Bewertungen
- Komatsu Hydraulic Excavator Pc290lc 290nlc 6k Shop ManualDokument20 SeitenKomatsu Hydraulic Excavator Pc290lc 290nlc 6k Shop Manualmallory100% (47)
- 7 CAAT-AIR-GM03 Guidance-Material-for-Foreign-Approved-Maintenance-Organization - I3R0 - 30oct2019 PDFDokument59 Seiten7 CAAT-AIR-GM03 Guidance-Material-for-Foreign-Approved-Maintenance-Organization - I3R0 - 30oct2019 PDFJindarat KasemsooksakulNoch keine Bewertungen
- Rotation and Revolution of EarthDokument4 SeitenRotation and Revolution of EarthRamu ArunachalamNoch keine Bewertungen
- Filipino Chicken Cordon BleuDokument7 SeitenFilipino Chicken Cordon BleuHazel Castro Valentin-VillamorNoch keine Bewertungen
- Powerpoints 4 4up8Dokument9 SeitenPowerpoints 4 4up8Ali KalyarNoch keine Bewertungen
- Sycip v. CA (Sufficient Funds With The Drawee Bank)Dokument15 SeitenSycip v. CA (Sufficient Funds With The Drawee Bank)Arnold BagalanteNoch keine Bewertungen
- ReportDokument8 SeitenReportTrust Asia Cargo in OfficeNoch keine Bewertungen
- What A Wonderful WorldDokument2 SeitenWhat A Wonderful WorldDraganaNoch keine Bewertungen
- Intimate TemporalitiesDokument12 SeitenIntimate TemporalitiesmittentenNoch keine Bewertungen
- A Comparison of Practitioner and Student WritingDokument28 SeitenA Comparison of Practitioner and Student WritingMichael Sniper WuNoch keine Bewertungen
- Title: Daily Visit Report: SDL Mini - Project Academic Year 2020-21 Group ID:GB6Dokument2 SeitenTitle: Daily Visit Report: SDL Mini - Project Academic Year 2020-21 Group ID:GB6Arjuna JppNoch keine Bewertungen
- WIKADokument10 SeitenWIKAPatnubay B TiamsonNoch keine Bewertungen
- Chap6 Part1Dokument15 SeitenChap6 Part1Francis Renjade Oafallas VinuyaNoch keine Bewertungen
- January Payslip 2023.pdf - 1-2Dokument1 SeiteJanuary Payslip 2023.pdf - 1-2Arbaz KhanNoch keine Bewertungen
- 1 Intro To Society, Community and EducationDokument29 Seiten1 Intro To Society, Community and EducationMaria Michelle A. Helar100% (1)
- PDF - Unpacking LRC and LIC Calculations For PC InsurersDokument14 SeitenPDF - Unpacking LRC and LIC Calculations For PC Insurersnod32_1206Noch keine Bewertungen
- Sorsogon State College: Republic of The Philippines Bulan Campus Bulan, SorsogonDokument4 SeitenSorsogon State College: Republic of The Philippines Bulan Campus Bulan, Sorsogonerickson hernanNoch keine Bewertungen
- 1 3 Quest-Answer 2014Dokument8 Seiten1 3 Quest-Answer 2014api-246595728Noch keine Bewertungen
- WRAP HandbookDokument63 SeitenWRAP Handbookzoomerfins220% (1)