Das könnte Ihnen auch gefallen
- Living on the Frontline of COVID-19 in MCO And CMCOVon EverandLiving on the Frontline of COVID-19 in MCO And CMCONoch keine Bewertungen
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19Von EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19Noch keine Bewertungen
- Immune Reconstitution Inflammatory Syndrome in HivDokument37 SeitenImmune Reconstitution Inflammatory Syndrome in Hivpokhara gharipatanNoch keine Bewertungen
- TB Hiv CoinfectionDokument29 SeitenTB Hiv CoinfectionVinobhachowdary DondapatiNoch keine Bewertungen
- TB-HIV Private PhysiciansDokument66 SeitenTB-HIV Private PhysiciansZulhelmiNoch keine Bewertungen
- Reconstituciòn InmuneDokument15 SeitenReconstituciòn InmuneMarialina PereiraNoch keine Bewertungen
- Nosocomial PneumoniasDokument103 SeitenNosocomial PneumoniasMuhammad Jahari SupiantoNoch keine Bewertungen
- 3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualDokument28 Seiten3 Pulmonary Fungal and Viral Infections Part 3 Viruses and UnusualjimmyneumologiaNoch keine Bewertungen
- HIV and Immune Reconstitution Inflammatory Syndrome HIV IRISDokument8 SeitenHIV and Immune Reconstitution Inflammatory Syndrome HIV IRISntnquynhproNoch keine Bewertungen
- HIV Neurology: Graeme MeintjesDokument75 SeitenHIV Neurology: Graeme MeintjesPrincess MiraNoch keine Bewertungen
- 03NTD 2022 - COVID-19 VS DengueDokument66 Seiten03NTD 2022 - COVID-19 VS DengueInstitute for Clinical ResearchNoch keine Bewertungen
- Immune Reconstitution InflammatoryDokument10 SeitenImmune Reconstitution InflammatoryBhanu KumarNoch keine Bewertungen
- Current Management of Fungal Urinary Tract Infection and FunguriaDokument47 SeitenCurrent Management of Fungal Urinary Tract Infection and FunguriaFeysel JemalNoch keine Bewertungen
- Laksmi - Pulmonary Aspect of HIV-AIDS and Its ManagementDokument45 SeitenLaksmi - Pulmonary Aspect of HIV-AIDS and Its ManagementNila hermawatiNoch keine Bewertungen
- IRIS SessionDokument41 SeitenIRIS SessionStela MonikaNoch keine Bewertungen
- Tuberculosis and The Immune Reconstitution Inflammatory Syndrome (IRIS)Dokument38 SeitenTuberculosis and The Immune Reconstitution Inflammatory Syndrome (IRIS)kung_pauNoch keine Bewertungen
- Bahan BacaanDokument21 SeitenBahan BacaanEka SatriawibawaNoch keine Bewertungen
- MKSAP 16 - Infectious DiseaseDokument340 SeitenMKSAP 16 - Infectious DiseaseBacanator75% (4)
- Immune Reconstitution Inflammatory Syndrome (Iris)Dokument6 SeitenImmune Reconstitution Inflammatory Syndrome (Iris)ashuNoch keine Bewertungen
- Sindrom Reconstructive ImunaDokument7 SeitenSindrom Reconstructive ImunaAlexandra PaunNoch keine Bewertungen
- PACE TrialDokument32 SeitenPACE TrialAppu EliasNoch keine Bewertungen
- The Immune Reconstitution Inflammatory SyndromeDokument7 SeitenThe Immune Reconstitution Inflammatory SyndromeAlexandra PaunNoch keine Bewertungen
- TB and HIVDokument43 SeitenTB and HIVNational Press FoundationNoch keine Bewertungen
- Clinical Management of TB and HIVDokument154 SeitenClinical Management of TB and HIVapi-3781623100% (3)
- Hiv / TB CollaborationDokument32 SeitenHiv / TB CollaborationFazlullah HashmiNoch keine Bewertungen
- Example of A Case Report-Cryptococcoal and IRISDokument5 SeitenExample of A Case Report-Cryptococcoal and IRISTorgbui Gorni Treve IVNoch keine Bewertungen
- Cip On CovidDokument40 SeitenCip On CovidLorenz L. Llamas IIINoch keine Bewertungen
- The Common Cases of Infectious Disease: An Approach To DiagnosisDokument29 SeitenThe Common Cases of Infectious Disease: An Approach To DiagnosisAlizaPinkyNoch keine Bewertungen
- Toxoplasmosis: Sugianto MukminDokument114 SeitenToxoplasmosis: Sugianto Mukmingiggs_libraNoch keine Bewertungen
- Management of Patients With Confirmed 2019-nCoV - CDCDokument9 SeitenManagement of Patients With Confirmed 2019-nCoV - CDCIndah BerlianaNoch keine Bewertungen
- Pneumonia in Critical Patients - KARTIKADokument29 SeitenPneumonia in Critical Patients - KARTIKAKartika JuwitaNoch keine Bewertungen
- Immune Reconstitution Syndrome (IRS)Dokument16 SeitenImmune Reconstitution Syndrome (IRS)Julian HuningkorNoch keine Bewertungen
- COVID-19 Home Based CareDokument26 SeitenCOVID-19 Home Based CareDineshani SirisenaNoch keine Bewertungen
- Immune Reconstitution Inflammatory SyndromeDokument8 SeitenImmune Reconstitution Inflammatory SyndromeRafif Abdurrahman WijisaksonoNoch keine Bewertungen
- Part 2 OI 26 JUN2018Dokument88 SeitenPart 2 OI 26 JUN2018Alimyon Abilar MontoloNoch keine Bewertungen
- 2.opportunistic Infections in HIV-infected PatientsDokument53 Seiten2.opportunistic Infections in HIV-infected PatientsAbebe TilahunNoch keine Bewertungen
- Disseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractDokument3 SeitenDisseminated Tuberculosis in An AIDS/HIV-Infected Patient: AbstractAmelia Fitria DewiNoch keine Bewertungen
- TB and HIV (Dr. E. Jane Carter)Dokument54 SeitenTB and HIV (Dr. E. Jane Carter)National Press FoundationNoch keine Bewertungen
- Original Article: Early-And Late-Onset Severe Pneumonia After Renal TransplantationDokument9 SeitenOriginal Article: Early-And Late-Onset Severe Pneumonia After Renal TransplantationAndra MariaNoch keine Bewertungen
- Baca Pustaka Respi AsniDokument26 SeitenBaca Pustaka Respi Asniasni_rahayu9020Noch keine Bewertungen
- 54 JMSCRDokument7 Seiten54 JMSCRVani Junior LoverzNoch keine Bewertungen
- Dr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InDokument76 SeitenDr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InAndry Wahyudi AgusNoch keine Bewertungen
- EtopxidoDokument28 SeitenEtopxidoNatalia ValenzuelaNoch keine Bewertungen
- Emergency MedDokument4 SeitenEmergency MedbencleeseNoch keine Bewertungen
- The Zelenko ProtocolDokument35 SeitenThe Zelenko ProtocolGoran KovacevicNoch keine Bewertungen
- Rickettsial InfectionsDokument45 SeitenRickettsial InfectionsTarikNoch keine Bewertungen
- Mycobacterial Infection:: Marshel Tendean, MD Department of Internal Medicine UKRIDA JakartaDokument36 SeitenMycobacterial Infection:: Marshel Tendean, MD Department of Internal Medicine UKRIDA Jakartaelevenia_emailNoch keine Bewertungen
- TB Guideline HivDokument6 SeitenTB Guideline HivArdi_xNoch keine Bewertungen
- Serum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusDokument29 SeitenSerum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusHadi SusilaNoch keine Bewertungen
- Essential Update: FDA Approves Rifapentine For Latent TB InfectionDokument16 SeitenEssential Update: FDA Approves Rifapentine For Latent TB InfectionAdriyan SikumalayNoch keine Bewertungen
- Boglione 2015Dokument9 SeitenBoglione 2015Thanh PhongNoch keine Bewertungen
- Common Opportunistic InfectionsDokument53 SeitenCommon Opportunistic InfectionsVeerapong VattanavanitNoch keine Bewertungen
- AHD & TB - ART Guidelines DisseminationDokument39 SeitenAHD & TB - ART Guidelines Disseminationfitness frixNoch keine Bewertungen
- CASE 4 FungalDokument14 SeitenCASE 4 FungalRhod SarNoch keine Bewertungen
- JC On TocilizumabDokument27 SeitenJC On TocilizumabNandha KumarNoch keine Bewertungen
- COVID - 19 Diagnosis - Current Updates FinalDokument63 SeitenCOVID - 19 Diagnosis - Current Updates FinalDr. Gurbilas P. SinghNoch keine Bewertungen
- Detection of Bacterial Infections Using PCT and CRP in Elderly Emergency Room PatientsDokument5 SeitenDetection of Bacterial Infections Using PCT and CRP in Elderly Emergency Room PatientsLydiaphNoch keine Bewertungen
- TB and HIVDokument43 SeitenTB and HIVNational Press Foundation100% (1)
- Presentation 1Dokument65 SeitenPresentation 1Lagath UdaraNoch keine Bewertungen
- Cap DR YuvaDokument169 SeitenCap DR YuvaYuvarajan SivaNoch keine Bewertungen
- 165 - 5.constipation in Patients With Spinal Cord InjuryDokument13 Seiten165 - 5.constipation in Patients With Spinal Cord InjuryKrittin NaravejsakulNoch keine Bewertungen
- 160 2.hepatolithiasis PDFDokument19 Seiten160 2.hepatolithiasis PDFKrittin NaravejsakulNoch keine Bewertungen
- 165 - 5.constipation in Patients With Spinal Cord InjuryDokument13 Seiten165 - 5.constipation in Patients With Spinal Cord InjuryKrittin NaravejsakulNoch keine Bewertungen
- 160 - 3.HP and NSAID Negative Peptic PDFDokument12 Seiten160 - 3.HP and NSAID Negative Peptic PDFKrittin NaravejsakulNoch keine Bewertungen
- 160 - 4.probiotics and Irritable Bowel PDFDokument15 Seiten160 - 4.probiotics and Irritable Bowel PDFKrittin NaravejsakulNoch keine Bewertungen
- 160 2.hepatolithiasis PDFDokument19 Seiten160 2.hepatolithiasis PDFKrittin NaravejsakulNoch keine Bewertungen
- Use of Vasopressors in Sepsis Resuscitation PDFDokument11 SeitenUse of Vasopressors in Sepsis Resuscitation PDFKrittin Naravejsakul100% (1)
- 160 - 4.probiotics and Irritable Bowel PDFDokument15 Seiten160 - 4.probiotics and Irritable Bowel PDFKrittin NaravejsakulNoch keine Bewertungen
- 160 - 4.probiotics and Irritable Bowel PDFDokument15 Seiten160 - 4.probiotics and Irritable Bowel PDFKrittin NaravejsakulNoch keine Bewertungen
- 165 - 5.constipation in Patients With Spinal Cord InjuryDokument13 Seiten165 - 5.constipation in Patients With Spinal Cord InjuryKrittin NaravejsakulNoch keine Bewertungen
- 160 - 3.HP and NSAID Negative Peptic PDFDokument12 Seiten160 - 3.HP and NSAID Negative Peptic PDFKrittin NaravejsakulNoch keine Bewertungen
- EyesDokument42 SeitenEyesKrittin NaravejsakulNoch keine Bewertungen
- 160 2.hepatolithiasis PDFDokument19 Seiten160 2.hepatolithiasis PDFKrittin NaravejsakulNoch keine Bewertungen
- 160 2.hepatolithiasis PDFDokument19 Seiten160 2.hepatolithiasis PDFKrittin NaravejsakulNoch keine Bewertungen
- Drug List-53 STDDokument24 SeitenDrug List-53 STDKrittin NaravejsakulNoch keine Bewertungen
- Definition of Terms2013Dokument80 SeitenDefinition of Terms2013Krittin NaravejsakulNoch keine Bewertungen
- Lecture Diarrhea and ConstipationDokument63 SeitenLecture Diarrhea and ConstipationKrittin NaravejsakulNoch keine Bewertungen
- °Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß °"√Æ‘‡§√"-Àåªí≠À"°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß„Π‡¥Á° ·Π«∑"ß°"√´-°ª√-«-Μ‘·≈-Μ√«®√À"ß°"¬ ‡§√◊Ëõß¡◊Õ ◊∫§Âπ∑"ß√-ß '«‘∑¬"·≈-‡«™»" Μ√Å𑫇§≈'¬√Å Tumor Markers °"√¬◊Π¬-Π°"√«‘Π‘®©-¬¢-Èπ Ÿ¥∑Â"¬Dokument40 Seiten°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß °"√Æ‘‡§√"-Àåªí≠À"°Âõπ∑Ÿ¡∫√‘‡«≥™Àõß∑Âõß„Π‡¥Á° ·Π«∑"ß°"√´-°ª√-«-Μ‘·≈-Μ√«®√À"ß°"¬ ‡§√◊Ëõß¡◊Õ ◊∫§Âπ∑"ß√-ß '«‘∑¬"·≈-‡«™»" Μ√Å𑫇§≈'¬√Å Tumor Markers °"√¬◊Π¬-Π°"√«‘Π‘®©-¬¢-Èπ Ÿ¥∑Â"¬priscillaNoch keine Bewertungen
- Electrolytes in PediatricsDokument84 SeitenElectrolytes in PediatricsKrittin NaravejsakulNoch keine Bewertungen
- PE Spine2010Dokument38 SeitenPE Spine2010Krittin NaravejsakulNoch keine Bewertungen
- ReA SittichaiDokument22 SeitenReA SittichaiKrittin NaravejsakulNoch keine Bewertungen
- Common Ent Emergencies 24126Dokument64 SeitenCommon Ent Emergencies 24126Krittin NaravejsakulNoch keine Bewertungen
- Pediatriccardiovascularproblemsinemergencysetting15 Feb 2011 110216224036 Phpapp02Dokument75 SeitenPediatriccardiovascularproblemsinemergencysetting15 Feb 2011 110216224036 Phpapp02Krittin NaravejsakulNoch keine Bewertungen
- Dementia and NeuropsychiatryDokument133 SeitenDementia and NeuropsychiatryKrittin Naravejsakul100% (1)
- EyesDokument42 SeitenEyesKrittin NaravejsakulNoch keine Bewertungen
- Ent Instruments 100503041754 Phpapp02Dokument59 SeitenEnt Instruments 100503041754 Phpapp02Krittin NaravejsakulNoch keine Bewertungen
- 191-Pitfalls in Management of Bleeding Disorders-20111117163513Dokument81 Seiten191-Pitfalls in Management of Bleeding Disorders-20111117163513Krittin NaravejsakulNoch keine Bewertungen
- Osce Ecg 110401044906 Phpapp01Dokument28 SeitenOsce Ecg 110401044906 Phpapp01Krittin NaravejsakulNoch keine Bewertungen
- Anticoagulants in AcsDokument66 SeitenAnticoagulants in AcsKrittin NaravejsakulNoch keine Bewertungen
- Micropara 1Dokument8 SeitenMicropara 1Jing DelfinNoch keine Bewertungen
- Daily Practice Test-25 (Zoology) Questions: Human Health and DiseaseDokument5 SeitenDaily Practice Test-25 (Zoology) Questions: Human Health and DiseaseShweta GajbhiyeNoch keine Bewertungen
- List of OIE DiseasesDokument5 SeitenList of OIE DiseasesShiva KhanalNoch keine Bewertungen
- Therapy of Acute Respiratory Infections in Children: NoveltiesDokument11 SeitenTherapy of Acute Respiratory Infections in Children: NoveltiesrizkaNoch keine Bewertungen
- Black DeathDokument6 SeitenBlack Deathapi-308366238Noch keine Bewertungen
- Pneumonia in Children What Is Pneumonia in Children?Dokument7 SeitenPneumonia in Children What Is Pneumonia in Children?Sandra GabasNoch keine Bewertungen
- Epidemiologi Penyakit TropisDokument36 SeitenEpidemiologi Penyakit TropisHusein RahmatNoch keine Bewertungen
- Edited 25 Agt 21-KOPI TB - Pengobatan TB Sensitif Obat Dan TB Resisten ObatDokument100 SeitenEdited 25 Agt 21-KOPI TB - Pengobatan TB Sensitif Obat Dan TB Resisten ObatAlvin Armando SantosoNoch keine Bewertungen
- Biology Investagotary ProjectDokument17 SeitenBiology Investagotary ProjectSumanthNoch keine Bewertungen
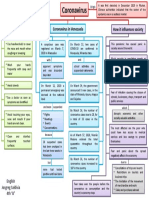
- Mapa Mental Coronavirus en InglesDokument1 SeiteMapa Mental Coronavirus en InglestavimayrNoch keine Bewertungen
- Emerging and Re-Emerging DiseasesDokument11 SeitenEmerging and Re-Emerging DiseasesJosielyn Valladolid0% (1)
- 481-Article Text-2650-1-10-20231016Dokument6 Seiten481-Article Text-2650-1-10-20231016indra yanaNoch keine Bewertungen
- Giardiasis - Causes, Symptoms, and TreatmentDokument9 SeitenGiardiasis - Causes, Symptoms, and TreatmentEmproNoch keine Bewertungen
- Mask Order 2021Dokument1 SeiteMask Order 2021Leah MoreauNoch keine Bewertungen
- Hand HygieneDokument8 SeitenHand HygieneQwequ Gong AnanseNoch keine Bewertungen
- MastitisDokument2 SeitenMastitisJuviely PremacioNoch keine Bewertungen
- Stenotrophomonas Maltophilia: Barry K. SeeboDokument10 SeitenStenotrophomonas Maltophilia: Barry K. SeeboBarry SeeboNoch keine Bewertungen
- Kode+Tarif RajalDokument8 SeitenKode+Tarif RajalroniNoch keine Bewertungen
- Health-Declaration-Checklist 2Dokument1 SeiteHealth-Declaration-Checklist 2Beverly Trangia100% (2)
- Standard PrecautionsDokument20 SeitenStandard PrecautionspomiakhterNoch keine Bewertungen
- Branching, Aerobic, Partially Acid Fast and Non-Acid Fast Gram (+) BacilliDokument2 SeitenBranching, Aerobic, Partially Acid Fast and Non-Acid Fast Gram (+) BacilliJustine Marie RevillaNoch keine Bewertungen
- Diagnosis and Treatment of Acute Tonsillopharyngitis A Guideline For Clinical PracticeDokument26 SeitenDiagnosis and Treatment of Acute Tonsillopharyngitis A Guideline For Clinical PracticeFX Fbs NewbieNoch keine Bewertungen
- Kuliah Pioderma DR Asih BudiastutiDokument56 SeitenKuliah Pioderma DR Asih BudiastutiunisoldierNoch keine Bewertungen
- Community Projectproposal Wash2Dokument3 SeitenCommunity Projectproposal Wash2Kenleinard ParafinaNoch keine Bewertungen
- Review Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Dokument26 SeitenReview Jurnal Varicella - Dewi Manik Aulia Fadli - 16700096Lia FadliNoch keine Bewertungen
- Cryptococcal Antigen Latex Agglutination Test JOSEPHDokument14 SeitenCryptococcal Antigen Latex Agglutination Test JOSEPHchocoholic potchiNoch keine Bewertungen
- Jabs2021AJO SUN Criterios HZV AUDokument9 SeitenJabs2021AJO SUN Criterios HZV AUNicolás Monteros AlviNoch keine Bewertungen
- Pemeriksaan Bakteriologis Lab TBDokument49 SeitenPemeriksaan Bakteriologis Lab TBTugas HeinzNoch keine Bewertungen
- Biology Investigatory Project: Malaria: Its Effects and CausesDokument17 SeitenBiology Investigatory Project: Malaria: Its Effects and CausesAnonymous XByxyTNoch keine Bewertungen
- Disease Vectors and Vector BionomicsDokument16 SeitenDisease Vectors and Vector BionomicsSuhas JoshiNoch keine Bewertungen