Das könnte Ihnen auch gefallen
- Healthy Lifestyle: Natural Tips to Live Healthy and Long - Ancient Health Tips and Techniques for a Healthy LifeVon EverandHealthy Lifestyle: Natural Tips to Live Healthy and Long - Ancient Health Tips and Techniques for a Healthy LifeNoch keine Bewertungen
- Megaloblastic Anemia: A Case StudyDokument30 SeitenMegaloblastic Anemia: A Case Studyromeo rivera100% (3)
- Case StudyDokument29 SeitenCase StudyGerome ValderamaNoch keine Bewertungen
- Physical Exam Reveals Nutrition and Gallstone Issues in FamilyDokument15 SeitenPhysical Exam Reveals Nutrition and Gallstone Issues in Familyriya haryaniNoch keine Bewertungen
- GORDONsDokument6 SeitenGORDONsNyj QuiñoNoch keine Bewertungen
- Age - For SubmissionDokument27 SeitenAge - For SubmissionAdrian MallarNoch keine Bewertungen
- Peptic Ulcer DiseaseDokument49 SeitenPeptic Ulcer DiseaseAngelie Sanchez86% (21)
- Case Study: Obstructive JaundiceDokument11 SeitenCase Study: Obstructive JaundiceZhy CaluzaNoch keine Bewertungen
- A Case Study On Preterm LaborDokument29 SeitenA Case Study On Preterm LaborBrexRomeoQuijada83% (18)
- Comprehensive Health History Output: Sam Albert J. RenaciaDokument7 SeitenComprehensive Health History Output: Sam Albert J. RenaciaSam Albert RenaciaNoch keine Bewertungen
- CKD Case PresentationDokument64 SeitenCKD Case PresentationGenevieve MundalaNoch keine Bewertungen
- Clinical Nutrition Conference VisionDokument29 SeitenClinical Nutrition Conference VisionMaya Rosmaria PNoch keine Bewertungen
- Acute Gastroenteritis (AGE) : A Case Study ONDokument28 SeitenAcute Gastroenteritis (AGE) : A Case Study ONCedy L. CieloNoch keine Bewertungen
- Celiac DseDokument50 SeitenCeliac DseJohn Christian LasalitaNoch keine Bewertungen
- Acute PyelonephritisDokument53 SeitenAcute Pyelonephritiseeymee100% (1)
- Preeclampsia: An OverviewDokument45 SeitenPreeclampsia: An OverviewYuri Iranda100% (1)
- Case StudyDokument27 SeitenCase StudyMikko Anthony Pingol AlarconNoch keine Bewertungen
- Nursing Process for Cardiovascular Disease PatientDokument56 SeitenNursing Process for Cardiovascular Disease PatientAra_Ongaco_8894Noch keine Bewertungen
- Appendicitis Signs and Symptoms GuideDokument40 SeitenAppendicitis Signs and Symptoms GuideHeart TolenadaNoch keine Bewertungen
- Acute Gastroenteritis (Age)Dokument37 SeitenAcute Gastroenteritis (Age)Jay Ar SantiagoNoch keine Bewertungen
- Final Case (Postpartum)Dokument14 SeitenFinal Case (Postpartum)KimJohnSanchoManeroNoch keine Bewertungen
- Case Analysis on Cholecystectomy CareDokument18 SeitenCase Analysis on Cholecystectomy CareAllyssa AnastacioNoch keine Bewertungen
- Ibn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"Dokument14 SeitenIbn-Sina Nursing and Midwifery Collage Case Study "Nursing Management"مالك مناصرةNoch keine Bewertungen
- Case Analysis on Cholecystectomy CareDokument18 SeitenCase Analysis on Cholecystectomy CareAllyssa AnastacioNoch keine Bewertungen
- Case Analysis on Cholecystectomy CareDokument18 SeitenCase Analysis on Cholecystectomy CareAllyssa AnastacioNoch keine Bewertungen
- Case 1 Amboss Abdominal PainDokument10 SeitenCase 1 Amboss Abdominal PainEstellaNoch keine Bewertungen
- Cadisal MW 1ST Week RequiementsDokument36 SeitenCadisal MW 1ST Week RequiementsJonathan GonzalesNoch keine Bewertungen
- Inflammation Gall Bladder Cholelithiasis Cystic Duct Inspissation Bile StasisDokument12 SeitenInflammation Gall Bladder Cholelithiasis Cystic Duct Inspissation Bile StasisAndrew Dela CruzNoch keine Bewertungen
- Tongson Yl8 PCGH Write-Up - AgeDokument7 SeitenTongson Yl8 PCGH Write-Up - AgeAlbert TongsonNoch keine Bewertungen
- Case Study SJH First SemDokument10 SeitenCase Study SJH First SemKathleen VargasNoch keine Bewertungen
- Case Study On Peptic Ulcer DiseaseDokument20 SeitenCase Study On Peptic Ulcer DiseaseYetTamparong50% (2)
- Case StudyDokument25 SeitenCase StudybomcorNoch keine Bewertungen
- Cyclic VomitingDokument19 SeitenCyclic VomitingEmily EresumaNoch keine Bewertungen
- I. Gordon'S Typology of 11 Health PatternsDokument5 SeitenI. Gordon'S Typology of 11 Health PatternsDan Ataniel EnsaladaNoch keine Bewertungen
- A Case Study On PuemoniaDokument32 SeitenA Case Study On Puemoniaxyzert100% (1)
- Patient Profile: AST Edical IstoryDokument9 SeitenPatient Profile: AST Edical IstoryAkocmeme SanchezNoch keine Bewertungen
- Klemanski - Abnormal Psy - RobertohandoutsDokument20 SeitenKlemanski - Abnormal Psy - Robertohandouts10yangb92Noch keine Bewertungen
- Case Study On FCBDDokument38 SeitenCase Study On FCBDKwinutskie LiteratoNoch keine Bewertungen
- Antenatal Case PresentationDokument10 SeitenAntenatal Case PresentationRijane Tabonoc OmlangNoch keine Bewertungen
- NRLE FORM - 05 Case Study of Lilian YuDokument4 SeitenNRLE FORM - 05 Case Study of Lilian YuJb RosillosaNoch keine Bewertungen
- Case in Herniorraphy BESTCASEDokument23 SeitenCase in Herniorraphy BESTCASEAdrian MallarNoch keine Bewertungen
- Typhoid FeverDokument38 SeitenTyphoid Fevermhamaenphapa27Noch keine Bewertungen
- Lumbar Compression Fracture: A Case StudyDokument46 SeitenLumbar Compression Fracture: A Case StudyOlivia SolomonNoch keine Bewertungen
- Acute Gastroenteritis (AGE) : A Case Study ONDokument9 SeitenAcute Gastroenteritis (AGE) : A Case Study ONMay Ann Magdaraog ArdamilNoch keine Bewertungen
- Takayasu'S Arteritis: A Case StudyDokument42 SeitenTakayasu'S Arteritis: A Case StudyErnesto Trinidad Jr RNNoch keine Bewertungen
- Nursing History I. Client's ProfileDokument6 SeitenNursing History I. Client's ProfileLc RamboyongNoch keine Bewertungen
- PELVIOLITHIASISDokument45 SeitenPELVIOLITHIASISAriane VidalNoch keine Bewertungen
- A Case StudyDokument51 SeitenA Case StudystansipekNoch keine Bewertungen
- Case AppendicitisDokument112 SeitenCase AppendicitisChen CobainNoch keine Bewertungen
- Functional Health PatternsDokument7 SeitenFunctional Health PatternsMeriam Angelita Robles AlfaroNoch keine Bewertungen
- NutritionalTherapy QuestionnaireDokument13 SeitenNutritionalTherapy Questionnairehalima mainaNoch keine Bewertungen
- Case Study On Pre EclampsiaDokument28 SeitenCase Study On Pre EclampsiaVianca Louriele Lavarro100% (3)
- NU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardDokument10 SeitenNU 665 Pediatric Gastrointestinal Case Study - Michelle - StewardMichelle StewardNoch keine Bewertungen
- H MoleDokument23 SeitenH MoleJoel Santos100% (1)
- Acute PyelonephritisDokument53 SeitenAcute Pyelonephritisverna96% (24)
- Gordon'S Functional Health Pattern: Client ProfileDokument6 SeitenGordon'S Functional Health Pattern: Client ProfileRainier Rhett ConchaNoch keine Bewertungen
- Case Study - OTITIS MEDIADokument9 SeitenCase Study - OTITIS MEDIAHasing Amado100% (1)
- Invest For Your HealthDokument36 SeitenInvest For Your HealthelenoNoch keine Bewertungen
- Fluids and Electrolytes AssignmentDokument16 SeitenFluids and Electrolytes Assignmentromeo riveraNoch keine Bewertungen
- Fundamentals of NursingDokument48 SeitenFundamentals of Nursinganon-429003100% (31)
- Coordination and Organizational DesignDokument37 SeitenCoordination and Organizational Designromeo rivera100% (1)
- Definition of AIDSDokument6 SeitenDefinition of AIDSromeo riveraNoch keine Bewertungen
- Paroxysmal Nocturnal Hemoglobinuria Case StudyDokument87 SeitenParoxysmal Nocturnal Hemoglobinuria Case Studyrachael100% (4)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Neurological Assessment - Romeo RiveraDokument9 SeitenNeurological Assessment - Romeo Riveraromeo riveraNoch keine Bewertungen
- Acid Base ImbalancesDokument24 SeitenAcid Base Imbalancesromeo riveraNoch keine Bewertungen
- A Creed For Those Who Have SufferedDokument1 SeiteA Creed For Those Who Have Sufferedromeo riveraNoch keine Bewertungen
- End of Shift ReportDokument2 SeitenEnd of Shift Reportromeo rivera100% (2)
- PaThoPhysiology of Ischemic CardiomyopathyDokument3 SeitenPaThoPhysiology of Ischemic Cardiomyopathyromeo riveraNoch keine Bewertungen
- Psychiatric Case StudyDokument32 SeitenPsychiatric Case Studyrachael85% (33)
- University of Eastern PhilippinesDokument7 SeitenUniversity of Eastern Philippinesromeo rivera100% (1)
- Newborn CareDokument55 SeitenNewborn Careromeo rivera100% (1)
- Fundamentals of Nursing Test IDokument22 SeitenFundamentals of Nursing Test IRose Ann100% (28)
- Practice Test Pediatric Nursing 100 ItemsDokument17 SeitenPractice Test Pediatric Nursing 100 ItemsPaul Christian P. Santos, RN94% (87)
- SH A Con AgeDokument4 SeitenSH A Con Ageromeo riveraNoch keine Bewertungen
- Case Study of A Patient With Ischemic CardiomyopathyDokument33 SeitenCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Pathology of Diabetic Ketoacidosis - Romeo Rivera Jr.Dokument1 SeitePathology of Diabetic Ketoacidosis - Romeo Rivera Jr.romeo riveraNoch keine Bewertungen
- Pa Tho Physiology of Meig's SyndromeDokument2 SeitenPa Tho Physiology of Meig's Syndromeromeo riveraNoch keine Bewertungen
- Airbourne PrecautionsDokument3 SeitenAirbourne PrecautionsnursetengNoch keine Bewertungen
- Medication AdministrationDokument13 SeitenMedication Administrationromeo rivera100% (1)
- R430-100-17. MEDICATIONS.: Rationale / ExplanationDokument5 SeitenR430-100-17. MEDICATIONS.: Rationale / Explanationromeo riveraNoch keine Bewertungen
- Strategies To Reduce Medication ErrorsDokument7 SeitenStrategies To Reduce Medication Errorsromeo riveraNoch keine Bewertungen
- Nursing 101 Facts About NursingDokument6 SeitenNursing 101 Facts About Nursingromeo riveraNoch keine Bewertungen
- Basic Surgical Techniques IllustratedDokument49 SeitenBasic Surgical Techniques Illustratedromeo rivera100% (3)
- Integrated Comprehensive TestDokument28 SeitenIntegrated Comprehensive Testromeo riveraNoch keine Bewertungen
- 9 Regions of The Abdominal CavityDokument1 Seite9 Regions of The Abdominal CavityBBCherriNoch keine Bewertungen
- Hepatobiliary System and Pancreas Pathology Situational AnalDokument20 SeitenHepatobiliary System and Pancreas Pathology Situational Analapi-3728522Noch keine Bewertungen
- Reversing Digestive MiseryDokument160 SeitenReversing Digestive MiseryVanessa Méril-Mamert100% (1)
- 2 Salivary GlandsDokument20 Seiten2 Salivary GlandsKaty SanchezNoch keine Bewertungen
- Anatomy of LiverDokument44 SeitenAnatomy of LiveryashodharaNoch keine Bewertungen
- Summary Notes - Topic 7 Human Nutrition - CIE Biology IGCSEDokument6 SeitenSummary Notes - Topic 7 Human Nutrition - CIE Biology IGCSEdavin gunawanNoch keine Bewertungen
- Balanced Diet and Factors that Influence Nutritional NeedsDokument11 SeitenBalanced Diet and Factors that Influence Nutritional NeedsRay PeramathevanNoch keine Bewertungen
- Biliary Tract Surgery in Dogs and CatsDokument5 SeitenBiliary Tract Surgery in Dogs and CatsEsther ArifinNoch keine Bewertungen
- Abdomen Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Dokument2 SeitenAbdomen Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Intan PradikaNoch keine Bewertungen
- حيا 211-215 دليل المعلمDokument171 Seitenحيا 211-215 دليل المعلم312qqqqppppNoch keine Bewertungen
- Ayurvedic Medicines For Liver Cirrhosis - Livclear - Fatty LiverDokument10 SeitenAyurvedic Medicines For Liver Cirrhosis - Livclear - Fatty LiverDr.Baldeep Kaur100% (1)
- Daftar Pasien Digest BornokDokument10 SeitenDaftar Pasien Digest BornokKelik WagiyantoNoch keine Bewertungen
- Anatomy & Physiology of SwallowingDokument6 SeitenAnatomy & Physiology of Swallowingbagir_dm10Noch keine Bewertungen
- Neonatal Intestinal Obstruction Causes, Symptoms, and TreatmentDokument21 SeitenNeonatal Intestinal Obstruction Causes, Symptoms, and TreatmentShahzad Bashir ShamsNoch keine Bewertungen
- Liver Function Test InterpretationDokument48 SeitenLiver Function Test InterpretationKiattipoom SukkulcharoenNoch keine Bewertungen
- Gastroenterology by Elagouri MohammedDokument31 SeitenGastroenterology by Elagouri MohammedStylesh GuRlyNoch keine Bewertungen
- WWW Kaizengastrocare Com Why Kaizen Gastro Care Is A One Stop Solution For All Gastro ProblemsDokument3 SeitenWWW Kaizengastrocare Com Why Kaizen Gastro Care Is A One Stop Solution For All Gastro ProblemsKaizen Gastro CareNoch keine Bewertungen
- Nursing Care Plan AmoebiasisDokument2 SeitenNursing Care Plan Amoebiasisderic97% (35)
- PBL 5.2 (Git 1)Dokument46 SeitenPBL 5.2 (Git 1)aiman mazlanNoch keine Bewertungen
- Digestive Systems: Regents BiologyDokument23 SeitenDigestive Systems: Regents BiologyJerrold MangaoNoch keine Bewertungen
- What is a gastrectomy surgeryDokument4 SeitenWhat is a gastrectomy surgeryPriyanka JangraNoch keine Bewertungen
- Human NutritionDokument18 SeitenHuman NutritionVeer RamloghunNoch keine Bewertungen
- Cholecystitis: What Is It?Dokument6 SeitenCholecystitis: What Is It?Aziil LiizaNoch keine Bewertungen
- Nursing Care Plan Cholecystectomy Gall Bladder RemovalDokument2 SeitenNursing Care Plan Cholecystectomy Gall Bladder Removalderic100% (16)
- Patient Instructions For Colonoscopy and Upper GI EndosDokument4 SeitenPatient Instructions For Colonoscopy and Upper GI EndosJm NitrileNoch keine Bewertungen
- General Stool ExaminationDokument6 SeitenGeneral Stool Examinationزكريا خالدNoch keine Bewertungen
- PancreatitisDokument26 SeitenPancreatitisJnah Macs100% (2)
- Cholelithiasis: Group MembersDokument12 SeitenCholelithiasis: Group MembersShiela GutierrezNoch keine Bewertungen
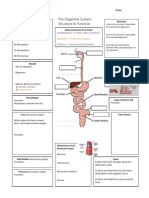
- The Digestive System Graphic OrganiserDokument1 SeiteThe Digestive System Graphic Organiserapi-350307578100% (1)
- Gastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Dokument11 SeitenGastric Versus Jejunal Feeding: Evidence or Emotion?: Nutrition Issues in Gastroenterology, Series #42Giselle Pezoa WattsonNoch keine Bewertungen