Das könnte Ihnen auch gefallen
- How Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887Dokument11 SeitenHow Bankruptcy Affects Real Estate Titles and Bankruptcy Risks Covered by Title Insurance - 00104887m1k0eNoch keine Bewertungen
- ATI CollaborationDokument46 SeitenATI Collaborationm1k0e72% (29)
- Monthly Membership Subscription FAQsDokument2 SeitenMonthly Membership Subscription FAQsm1k0eNoch keine Bewertungen
- LicenseDokument7 SeitenLicenseAdnan AvdukićNoch keine Bewertungen
- Osteoarthritis, Hip Replacement, OsteoporosisDokument19 SeitenOsteoarthritis, Hip Replacement, Osteoporosism1k0eNoch keine Bewertungen
- MGMT E-2000 Fall 2014 SyllabusDokument13 SeitenMGMT E-2000 Fall 2014 Syllabusm1k0eNoch keine Bewertungen
- ATIpendixDokument38 SeitenATIpendixm1k0e100% (1)
- Ati Codes Cont'Dokument1 SeiteAti Codes Cont'm1k0eNoch keine Bewertungen
- Hyponatremia: Symptoms May Vary With Changes in Vascular VolumeDokument3 SeitenHyponatremia: Symptoms May Vary With Changes in Vascular Volumem1k0eNoch keine Bewertungen
- HTN - Sodium PPT EditionDokument15 SeitenHTN - Sodium PPT Editionm1k0eNoch keine Bewertungen
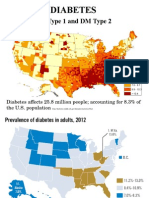
- Endo DM Type 1 and 2Dokument35 SeitenEndo DM Type 1 and 2m1k0eNoch keine Bewertungen
- IV medication reconstitution checklistDokument3 SeitenIV medication reconstitution checklistm1k0eNoch keine Bewertungen
- Health & Physical Assessment in Nursing: Donita D'Amico Colleen BarbaritoDokument48 SeitenHealth & Physical Assessment in Nursing: Donita D'Amico Colleen Barbaritom1k0eNoch keine Bewertungen
- Introduction To Pediatric Nursing 2012 Student VersionDokument71 SeitenIntroduction To Pediatric Nursing 2012 Student Versionm1k0eNoch keine Bewertungen
- Antimicrobial Stewardship: Attempting To Preserve A Strategic ResourceDokument7 SeitenAntimicrobial Stewardship: Attempting To Preserve A Strategic Resourcem1k0eNoch keine Bewertungen
- EKG Crash Course NuRsing 390 SMC - 4Dokument57 SeitenEKG Crash Course NuRsing 390 SMC - 4m1k0e100% (2)
- HTN - Sodium PPT EditionDokument15 SeitenHTN - Sodium PPT Editionm1k0eNoch keine Bewertungen
- Medicine American Journal of Hospice and PalliativeDokument6 SeitenMedicine American Journal of Hospice and Palliativem1k0eNoch keine Bewertungen
- Reducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current PerspectivesDokument13 SeitenReducing Inappropriate Antibiotic Prescribing in The Residential Care Setting: Current Perspectivesm1k0eNoch keine Bewertungen
- The Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of LifeDokument4 SeitenThe Pattern of Antimicrobial Use For Palliative Care In-Patients During The Last Week of Lifem1k0eNoch keine Bewertungen
- Mus Culo Skeletal Exam OutlineDokument14 SeitenMus Culo Skeletal Exam Outlinem1k0eNoch keine Bewertungen
- Hesi Entrance Examination Study GuideDokument195 SeitenHesi Entrance Examination Study Guidetken35100% (2)
- Obtaining A Pap SmearDokument1 SeiteObtaining A Pap Smearm1k0eNoch keine Bewertungen
- Effectiveness of A Comprehensive Hand Hygiene Program ForDokument11 SeitenEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNoch keine Bewertungen
- Effectiveness of A Comprehensive Hand Hygiene Program ForDokument11 SeitenEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNoch keine Bewertungen
- Chapter 003Dokument2 SeitenChapter 003m1k0eNoch keine Bewertungen
- Guide To UspsDokument28 SeitenGuide To Uspsm1k0eNoch keine Bewertungen
- Atoal Material Safety Data SheetsDokument1 SeiteAtoal Material Safety Data Sheetsm1k0eNoch keine Bewertungen
- Chapter 3 Macromolecules and The Origin of LifeDokument13 SeitenChapter 3 Macromolecules and The Origin of Lifem1k0eNoch keine Bewertungen
- 7211 Vitamin K 2014Dokument42 Seiten7211 Vitamin K 2014m1k0eNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Chronic Injury ManagementDokument19 SeitenChronic Injury ManagementHANZEL JUDE PIMENTELNoch keine Bewertungen
- Ketu Effects and RemediesDokument4 SeitenKetu Effects and RemediesSumitasNoch keine Bewertungen
- Referral Letter: Client Personal Details Client Identity DetailsDokument2 SeitenReferral Letter: Client Personal Details Client Identity DetailsFlorence LinNoch keine Bewertungen
- Reproductive Health New BioHack - 339c99f5 F05a 4b5f A8e3 29479f745555Dokument7 SeitenReproductive Health New BioHack - 339c99f5 F05a 4b5f A8e3 29479f745555Adamya Tyagi X-ANoch keine Bewertungen
- Fitness Calculator Python ProjectDokument12 SeitenFitness Calculator Python ProjectNishitha NeelamNoch keine Bewertungen
- Combination of Curcumin-β-Cyclodextrin and Aloe vera for lowering Mouth Ulcers in Acetic Acid Induced Rats ModelDokument10 SeitenCombination of Curcumin-β-Cyclodextrin and Aloe vera for lowering Mouth Ulcers in Acetic Acid Induced Rats ModelSutriyo Abdullah100% (1)
- Assignment No 04Dokument2 SeitenAssignment No 04Muskan FatimaNoch keine Bewertungen
- Medication Dialogue: Obs. in Loc de How Are You Feeling?", Putem Folosi How Do You Feel?", Fara Sa SchimbamDokument4 SeitenMedication Dialogue: Obs. in Loc de How Are You Feeling?", Putem Folosi How Do You Feel?", Fara Sa SchimbamToma GeorgianaaNoch keine Bewertungen
- Tourniquet Application During AnesthesiaDokument7 SeitenTourniquet Application During AnesthesiaaksinuNoch keine Bewertungen
- LIC Jeevan Shiromani 9 Inch X 8 Inch EngDokument22 SeitenLIC Jeevan Shiromani 9 Inch X 8 Inch EngNithin KKNoch keine Bewertungen
- Fundamentals Nursing The Art and Science of Nursing Care 7th Edition Taylor Test BankDokument8 SeitenFundamentals Nursing The Art and Science of Nursing Care 7th Edition Taylor Test BankGeorgeCobbjgbcs100% (15)
- Ayurvedic Management of DiseasesDokument25 SeitenAyurvedic Management of DiseasesShreyaNoch keine Bewertungen
- Kulkarni 2016 PDFDokument21 SeitenKulkarni 2016 PDFquirinalNoch keine Bewertungen
- Duo Max bactericidal efficacy assessmentDokument7 SeitenDuo Max bactericidal efficacy assessmentAllen Wei ChnugNoch keine Bewertungen
- Antimicrobial Properties of Coconut Shell OilDokument12 SeitenAntimicrobial Properties of Coconut Shell OilBalakrishna GopinathNoch keine Bewertungen
- Bedbugs Punaises Lits EngDokument2 SeitenBedbugs Punaises Lits EngMohammad Faizul Haque KhanNoch keine Bewertungen
- Percutaneous Transluminal Coronary AngioplastyDokument22 SeitenPercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)
- Unusual respiratory failure after caustic ingestionDokument4 SeitenUnusual respiratory failure after caustic ingestionRay MaudyNoch keine Bewertungen
- Eduskills Listening Mock Test Day 3 QNDokument15 SeitenEduskills Listening Mock Test Day 3 QNselvarajmarithai1432Noch keine Bewertungen
- Tibetan Demons PDFDokument30 SeitenTibetan Demons PDFLázaro OmenaNoch keine Bewertungen
- (PIH) CASE PRESENTATION (Group11)Dokument41 Seiten(PIH) CASE PRESENTATION (Group11)Kaye Drexcel SequilloNoch keine Bewertungen
- Swallowing Swallowing: Person-Centered Focus On Function: Person-Centered Focus On FunctionDokument2 SeitenSwallowing Swallowing: Person-Centered Focus On Function: Person-Centered Focus On FunctionGabriel MoralesNoch keine Bewertungen
- NCP JaundiceDokument3 SeitenNCP Jaundiceanilobaid84% (25)
- Chapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokument7 SeitenChapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNoch keine Bewertungen
- Standardizing Urine Conditions for NMR Metabolomics StudiesDokument24 SeitenStandardizing Urine Conditions for NMR Metabolomics StudiesJessicaNoch keine Bewertungen
- Labour Presentation ObsDokument48 SeitenLabour Presentation ObsVera BannorNoch keine Bewertungen
- Postpartum DepressionDokument3 SeitenPostpartum DepressionMelanie GaledoNoch keine Bewertungen
- Lec 12 - Drugs Used in PTDokument14 SeitenLec 12 - Drugs Used in PTAiqa QaziNoch keine Bewertungen
- 29 Days Study Plan and Important Stuff by Hafiz Bilal For 4TH Year MBBS PDFDokument3 Seiten29 Days Study Plan and Important Stuff by Hafiz Bilal For 4TH Year MBBS PDFDaneyal Arshad100% (2)
- Visiting the Market During COVID LockdownDokument1 SeiteVisiting the Market During COVID LockdownMuhammad Awais Hassan AwaanNoch keine Bewertungen