Das könnte Ihnen auch gefallen
- RS80 EVO Reference Manual En-UsDokument292 SeitenRS80 EVO Reference Manual En-UskarenNoch keine Bewertungen
- Cyanotic Heart DiseaseDokument47 SeitenCyanotic Heart Disease87-Saranya MNoch keine Bewertungen
- AIIMS PG Brochure - Jul 20 PDFDokument83 SeitenAIIMS PG Brochure - Jul 20 PDFSurya50% (2)
- Obstetrics MCQsDokument28 SeitenObstetrics MCQsMenna KamalNoch keine Bewertungen
- Doppler InjuryDokument38 SeitenDoppler InjuryRachel SissonNoch keine Bewertungen
- Fetal Doppler Assessment in PregnancyDokument40 SeitenFetal Doppler Assessment in PregnancyKEN KIZITONoch keine Bewertungen
- Update of Fetal Growth Restriction: I Nyoman Suetri TapayanaDokument44 SeitenUpdate of Fetal Growth Restriction: I Nyoman Suetri TapayanatapayanaNoch keine Bewertungen
- DOPPLER ULTRASOUND IN PREGNANCYDokument64 SeitenDOPPLER ULTRASOUND IN PREGNANCYHerry SasukeNoch keine Bewertungen
- Penyakit Jantung Bawaan - IDokument44 SeitenPenyakit Jantung Bawaan - IEkisliefvirjou Adelihira HidraNoch keine Bewertungen
- Biophysical Profile& Color Doppler Ultrasound in The High Risk PregnancyDokument56 SeitenBiophysical Profile& Color Doppler Ultrasound in The High Risk Pregnancykhadzx100% (4)
- Fetal Growth Restriction UGDokument50 SeitenFetal Growth Restriction UGBrutus AntonyNoch keine Bewertungen
- Anaesthetic Management in Obstetric Haemorrhage: DR B.Srikanth Iindyrpg Dept. of AnaesthesiaDokument34 SeitenAnaesthetic Management in Obstetric Haemorrhage: DR B.Srikanth Iindyrpg Dept. of AnaesthesiaEDI CNoch keine Bewertungen
- Anaesthetic Management of Congenital Heart DiseasesDokument56 SeitenAnaesthetic Management of Congenital Heart DiseasesShehan WijayasiriwardanaNoch keine Bewertungen
- CTSU Presentation PDADokument41 SeitenCTSU Presentation PDAEdwin OkonNoch keine Bewertungen
- Obstetrics: Physiologic Changes of PregnancyDokument6 SeitenObstetrics: Physiologic Changes of Pregnancyapi-3829364Noch keine Bewertungen
- Dr. IkhsanDokument46 SeitenDr. IkhsanandiendaNoch keine Bewertungen
- Maternal Physiology in Pregnancy by ERMIDokument56 SeitenMaternal Physiology in Pregnancy by ERMIHenok Y KebedeNoch keine Bewertungen
- CTG & DopplerDokument40 SeitenCTG & DopplerSara BatistaNoch keine Bewertungen
- Dr. Shaker's Guide to Managing Cyanotic Heart DiseaseDokument66 SeitenDr. Shaker's Guide to Managing Cyanotic Heart DiseasePrasanth SankarNoch keine Bewertungen
- Pulmonary Atresia With Ventricular Septal DefectDokument23 SeitenPulmonary Atresia With Ventricular Septal Defectluulamthangtai0105Noch keine Bewertungen
- Cardiac Effusions: Causes, Symptoms and DiagnosisDokument26 SeitenCardiac Effusions: Causes, Symptoms and DiagnosisjsenocNoch keine Bewertungen
- 28b- EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020Dokument8 Seiten28b- EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020saeed hasan saeedNoch keine Bewertungen
- Physiologic Changes in PregDokument36 SeitenPhysiologic Changes in PregTadesse MuhammedNoch keine Bewertungen
- Absent End DiastolicDokument12 SeitenAbsent End DiastolicAndre PutraNoch keine Bewertungen
- PdaDokument43 SeitenPdaSandy ShahNoch keine Bewertungen
- Coarctation of Aorta: Seoul National University Hospital Department of Thoracic & Cardiovascular SurgeryDokument39 SeitenCoarctation of Aorta: Seoul National University Hospital Department of Thoracic & Cardiovascular Surgeryprencess_jeny5006Noch keine Bewertungen
- Doppler US and GrowthDokument43 SeitenDoppler US and GrowthAulia rahmawatiNoch keine Bewertungen
- Physiological Adaptations during Pregnancy, Labor, and Early Postpartum (39Dokument39 SeitenPhysiological Adaptations during Pregnancy, Labor, and Early Postpartum (39Kevin NugrohoNoch keine Bewertungen
- Changes in Cardiovascular System During PostpartumDokument12 SeitenChanges in Cardiovascular System During PostpartumKpiebakyene Sr. MercyNoch keine Bewertungen
- 3881825Dokument30 Seiten3881825saryindrianyNoch keine Bewertungen
- (I..) KMU Peads CardicDokument88 Seiten(I..) KMU Peads CardicMuhammadNoch keine Bewertungen
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDokument69 SeitenUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNoch keine Bewertungen
- Right Superior Vena Cava Draining To Left AtriumDokument42 SeitenRight Superior Vena Cava Draining To Left AtriumKunwar Sidharth SaurabhNoch keine Bewertungen
- Cardiac Disease in PregnancyDokument86 SeitenCardiac Disease in PregnancyAustine OdhiamboNoch keine Bewertungen
- Chronic Renal Failure During PregnancyDokument42 SeitenChronic Renal Failure During PregnancyvincentsharonNoch keine Bewertungen
- Cyanotic Congenital Heart DiseasesDokument25 SeitenCyanotic Congenital Heart DiseasesAlvin OmondiNoch keine Bewertungen
- Fluid Resuscitation and Volume Assessment: - Does This Patient Have Adequate Organ Perfusion?Dokument24 SeitenFluid Resuscitation and Volume Assessment: - Does This Patient Have Adequate Organ Perfusion?RichardNoch keine Bewertungen
- VSD Types, Causes, Symptoms, and TreatmentDokument18 SeitenVSD Types, Causes, Symptoms, and TreatmentnoekkuNoch keine Bewertungen
- Obstetrics V13 Obstetric Emergencies Chapter Diagnosis and Management of Shock in Postpartum Hemorrhage 1682196492Dokument14 SeitenObstetrics V13 Obstetric Emergencies Chapter Diagnosis and Management of Shock in Postpartum Hemorrhage 1682196492lizzieNoch keine Bewertungen
- Patent Ductus Arteriosus in Preterm Neonates: DR Deepti Damayanty Pradhan KIMS, BhubaneswarDokument58 SeitenPatent Ductus Arteriosus in Preterm Neonates: DR Deepti Damayanty Pradhan KIMS, BhubaneswarDr.Sushree Smita BehuraNoch keine Bewertungen
- Tekanan IntrakranialDokument20 SeitenTekanan IntrakranialHendra SupriawanNoch keine Bewertungen
- Heart disease in pregnancyDokument87 SeitenHeart disease in pregnancyMonisha ArulalanNoch keine Bewertungen
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDokument65 SeitenHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNoch keine Bewertungen
- Patent Ductus Arteriosu1Dokument2 SeitenPatent Ductus Arteriosu1AisyahKautsarIlmiNoch keine Bewertungen
- Cardio My Opa ThiesDokument73 SeitenCardio My Opa Thiesriyazadsumaiyajb2003Noch keine Bewertungen
- Transposition of The Great ArteriesDokument17 SeitenTransposition of The Great ArteriesGaram Esther GohNoch keine Bewertungen
- Pregnancy & Its Anaesthetic ImplicationsDokument29 SeitenPregnancy & Its Anaesthetic ImplicationsDadik WijayaNoch keine Bewertungen
- Maternal Physiology During PregnancyDokument60 SeitenMaternal Physiology During PregnancySerge TresorNoch keine Bewertungen
- Cardio Vascular Disease in PregnancyDokument57 SeitenCardio Vascular Disease in PregnancySanthosh.S.U0% (1)
- Congenital Heart DefectsDokument73 SeitenCongenital Heart DefectsStaen KisNoch keine Bewertungen
- Case Scenerio: DR Sourath Munir Malkani Fcps-Ii TraineDokument31 SeitenCase Scenerio: DR Sourath Munir Malkani Fcps-Ii TraineSoonh ChannaNoch keine Bewertungen
- ucu-CHDs_240114_230618 (2)Dokument68 Seitenucu-CHDs_240114_230618 (2)BrianNoch keine Bewertungen
- Antenatal Assessment of Fetal WellbeingDokument52 SeitenAntenatal Assessment of Fetal Wellbeing6ixSideCreate MNoch keine Bewertungen
- Pulmonary Hemorrhage: Dr. Habibur RahimDokument46 SeitenPulmonary Hemorrhage: Dr. Habibur Rahimallaaobeid1987Noch keine Bewertungen
- Dr. Maulik Vaja Moderator: Dr. C. S. NAIDUDokument106 SeitenDr. Maulik Vaja Moderator: Dr. C. S. NAIDUDilip Kumar MNoch keine Bewertungen
- Acyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianDokument98 SeitenAcyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianVijayakanth VijayakumarNoch keine Bewertungen
- Pregnancy and HeartDokument53 SeitenPregnancy and HeartgibreilNoch keine Bewertungen
- Intrauterine Growth RestrictionDokument8 SeitenIntrauterine Growth Restrictionmalgosia7Noch keine Bewertungen
- Diagnosis and Management of Shock in Postpartum HemorrhageDokument12 SeitenDiagnosis and Management of Shock in Postpartum HemorrhageJeferson CuaranNoch keine Bewertungen
- Master File 2003 - Body As A WholeDokument32 SeitenMaster File 2003 - Body As A Wholeobinna12Noch keine Bewertungen
- Uterine FibroidsDokument46 SeitenUterine FibroidsErwynsonsaut SimanjuntakNoch keine Bewertungen
- The Female Reproductive SystemDokument42 SeitenThe Female Reproductive SystemErwynsonsaut SimanjuntakNoch keine Bewertungen
- ICD X dan ICD IX CM Hubungan Dengan CasemixDokument67 SeitenICD X dan ICD IX CM Hubungan Dengan CasemixErwynsonsaut SimanjuntakNoch keine Bewertungen
- Postnatal DepressionDokument11 SeitenPostnatal DepressionErwynsonsaut SimanjuntakNoch keine Bewertungen
- WHO FHE MSM 94.11 Rev.1 PDFDokument114 SeitenWHO FHE MSM 94.11 Rev.1 PDFErwynsonsaut SimanjuntakNoch keine Bewertungen
- Prelabour Rupture of Membranes ManagementDokument9 SeitenPrelabour Rupture of Membranes ManagementErwynsonsaut SimanjuntakNoch keine Bewertungen
- HIV Dengan Infeksi Oportunistik Yudianto PIT Feto Mar 032015 Final - Yudianto PDFDokument34 SeitenHIV Dengan Infeksi Oportunistik Yudianto PIT Feto Mar 032015 Final - Yudianto PDFErwynsonsaut SimanjuntakNoch keine Bewertungen
- Ovariancysts 150512151145 Lva1 App6892Dokument28 SeitenOvariancysts 150512151145 Lva1 App6892Erwynsonsaut SimanjuntakNoch keine Bewertungen
- Pengenalan Kepada Icdxdanicdixcm: Nutrul AkbarDokument69 SeitenPengenalan Kepada Icdxdanicdixcm: Nutrul AkbarErwynsonsaut SimanjuntakNoch keine Bewertungen
- LC5C5PRO BUM 5268596-100 Rev A.bookDokument891 SeitenLC5C5PRO BUM 5268596-100 Rev A.bookErwynsonsaut Simanjuntak100% (1)
- 2015 Dga TimelineDokument1 Seite2015 Dga TimelineErwynsonsaut SimanjuntakNoch keine Bewertungen
- 7161Dokument22 Seiten7161Erwynsonsaut SimanjuntakNoch keine Bewertungen
- Appendix A Contents New ManualDokument12 SeitenAppendix A Contents New ManualErwynsonsaut SimanjuntakNoch keine Bewertungen
- LC5C5PRO BUM 5268596-100 Rev A.bookDokument891 SeitenLC5C5PRO BUM 5268596-100 Rev A.bookErwynsonsaut Simanjuntak100% (1)
- Calligraphy Dover BeachDokument1 SeiteCalligraphy Dover BeachErwynsonsaut SimanjuntakNoch keine Bewertungen
- Breast CancerDokument38 SeitenBreast CancerojoayodeleNoch keine Bewertungen
- 15b Ectopicpregnancy 090507104012 Phpapp02 130825152041 Phpapp01Dokument48 Seiten15b Ectopicpregnancy 090507104012 Phpapp02 130825152041 Phpapp01Erwynsonsaut SimanjuntakNoch keine Bewertungen
- 7Dokument45 Seiten7Erwynsonsaut SimanjuntakNoch keine Bewertungen
- 27cardiopulmonary GI2006Dokument8 Seiten27cardiopulmonary GI2006Erwynsonsaut SimanjuntakNoch keine Bewertungen
- Appendicitis Pregnancy ElnasharDokument47 SeitenAppendicitis Pregnancy ElnasharErwynsonsaut SimanjuntakNoch keine Bewertungen
- Hyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundDokument22 SeitenHyperthyroidism, Thyroid Storm, and Graves Disease: BackgroundAnonymous 3OoumAUytNoch keine Bewertungen
- Every Newborn: Spotlight On PhilippinesDokument8 SeitenEvery Newborn: Spotlight On PhilippinesRia Tiglao FortugalizaNoch keine Bewertungen
- Intraoperative Fluid ManagementDokument15 SeitenIntraoperative Fluid ManagementMirela Marina BlajNoch keine Bewertungen
- LoaDokument4 SeitenLoaYudistira WardanaNoch keine Bewertungen
- ASD Pathophysiology, Signs, Symptoms, and TreatmentDokument1 SeiteASD Pathophysiology, Signs, Symptoms, and TreatmentMSNoch keine Bewertungen
- Peripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemDokument70 SeitenPeripheral Nerve Injuries: Nerve Connective Tissue Nervous SystemRupika SodhiNoch keine Bewertungen
- Essential Oil Safety Cheatsheet Updated 2Dokument1 SeiteEssential Oil Safety Cheatsheet Updated 2Silvia De Alejandro100% (1)
- Czasopisma Lista MinisterialnaDokument318 SeitenCzasopisma Lista Ministerialnaarmach23Noch keine Bewertungen
- Asomacon 2023Dokument2 SeitenAsomacon 2023sindeeNoch keine Bewertungen
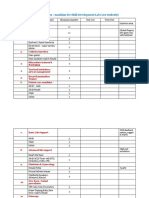
- Manikins Proposed List For Skill LabDokument3 SeitenManikins Proposed List For Skill LabNaren KNoch keine Bewertungen
- Implant JadelleDokument22 SeitenImplant JadelleIrma Amalia100% (1)
- 2017 Psgs Accreditation ManualDokument75 Seiten2017 Psgs Accreditation ManualJhessie ChingNoch keine Bewertungen
- Paediatric Imaging Guidelines - FinDokument7 SeitenPaediatric Imaging Guidelines - FinValencius SunandarNoch keine Bewertungen
- Somera CaseDokument2 SeitenSomera CaseShena LizaNoch keine Bewertungen
- Production and Operations Management: Massachusetts General Hospital's Pre-Admission Testing Area PATA Case StudyDokument10 SeitenProduction and Operations Management: Massachusetts General Hospital's Pre-Admission Testing Area PATA Case StudyJoaquín Norambuena EscalonaNoch keine Bewertungen
- Shoulder Impingement SyndromeDokument37 SeitenShoulder Impingement SyndromeDADDYGUS100% (1)
- Critical Evaluation of Nursing ProgrammeDokument31 SeitenCritical Evaluation of Nursing ProgrammeManoj Garg86% (14)
- Ultrasound Detected Ovarian Cysts For Nuh Gynaecology TeamsDokument11 SeitenUltrasound Detected Ovarian Cysts For Nuh Gynaecology TeamsDirga Rasyidin LNoch keine Bewertungen
- Clinical Practice Guidelines 11-18Dokument20 SeitenClinical Practice Guidelines 11-18Feroz RaZa SoomrOoNoch keine Bewertungen
- Resident On Call PDFDokument143 SeitenResident On Call PDFMuhammad RezaNoch keine Bewertungen
- Alternative Method For Fabrication of Power ArmDokument2 SeitenAlternative Method For Fabrication of Power ArmVikas VatsNoch keine Bewertungen
- Hook Surgery Practice Booklet PDFDokument4 SeitenHook Surgery Practice Booklet PDFAnonymous b9RIEMekNoch keine Bewertungen
- Cataract Art - Science - PDFDokument405 SeitenCataract Art - Science - PDFNidia M. Quispe RodríguezNoch keine Bewertungen
- Rajesh Neuro CenterDokument2 SeitenRajesh Neuro Centerrajesh neuroNoch keine Bewertungen
- Evidence Based PediatricDokument463 SeitenEvidence Based Pediatricsetyo pranotoNoch keine Bewertungen
- Instruction Manual SENDO Advance EnglishDokument17 SeitenInstruction Manual SENDO Advance EnglishАпарати за кръвно налягане SendoNoch keine Bewertungen
- Trauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiDokument39 SeitenTrauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiAtika SugiartoNoch keine Bewertungen