Das könnte Ihnen auch gefallen
- Sfss TurkeyDokument68 SeitenSfss TurkeytasarimkutusuNoch keine Bewertungen
- Newnes Electronics Circuits Pocket Book (Linear IC): Newnes Electronics Circuits Pocket Book, Volume 1Von EverandNewnes Electronics Circuits Pocket Book (Linear IC): Newnes Electronics Circuits Pocket Book, Volume 1Bewertung: 4.5 von 5 Sternen4.5/5 (3)
- Fluid TherapiDokument158 SeitenFluid TherapiAsmalina AzizanNoch keine Bewertungen
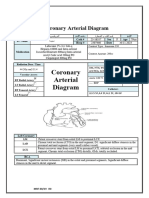
- Coronary Arterial DiagramDokument4 SeitenCoronary Arterial Diagramshamaamo19Noch keine Bewertungen
- Sysmex KX 21 Histogram Interpretation HandbookDokument28 SeitenSysmex KX 21 Histogram Interpretation Handbookسعد الطائع100% (4)
- Scenario Summary: Changing CellsDokument10 SeitenScenario Summary: Changing CellsMBA/2022/1474 AYUSHI ADWANINoch keine Bewertungen
- Martin - Steps To Achieve Abdominal MRI OptimizationDokument23 SeitenMartin - Steps To Achieve Abdominal MRI OptimizationrenatafisicamNoch keine Bewertungen
- Electrolytes Water Balance PH Balance Trace MetalsDokument21 SeitenElectrolytes Water Balance PH Balance Trace MetalsJohn Kevin Carl SaligumbaNoch keine Bewertungen
- Plennary Lecture Prof. Lukman - Transplantasi Jantung-OkDokument18 SeitenPlennary Lecture Prof. Lukman - Transplantasi Jantung-OkRiana AndardewiNoch keine Bewertungen
- Primary PCI To LAD and LCXDokument3 SeitenPrimary PCI To LAD and LCXshamaamo19Noch keine Bewertungen
- Coronary Arterial DiagramDokument3 SeitenCoronary Arterial Diagramshamaamo19Noch keine Bewertungen
- Report PDFDokument3 SeitenReport PDFPrancy PatelNoch keine Bewertungen
- TN KoesrinDokument5 SeitenTN KoesrinCristian RajagukgukNoch keine Bewertungen
- Clinico-Pathologic ConferenceDokument4 SeitenClinico-Pathologic ConferenceMichael ValderramaNoch keine Bewertungen
- Analyzed ResultsDokument8 SeitenAnalyzed ResultsSir BucketheadNoch keine Bewertungen
- BPH Lab and DiagnosticsDokument27 SeitenBPH Lab and DiagnosticsKceey CruzNoch keine Bewertungen
- Acute Renal Failure: An UpdateDokument52 SeitenAcute Renal Failure: An Updatepranav1512Noch keine Bewertungen
- Assessment of Left AtriumDokument68 SeitenAssessment of Left Atriumadh30Noch keine Bewertungen
- b0907 HowDokument50 Seitenb0907 HowyamtotlNoch keine Bewertungen
- Hand Out X-Class Masurement PrinciplesDokument10 SeitenHand Out X-Class Masurement PrinciplesJovan JovicNoch keine Bewertungen
- Cardiac Cath FinalDokument3 SeitenCardiac Cath Finalshamaamo19Noch keine Bewertungen
- CBC Test Name Result Result Result Result Reference Range August 21, 2021 August 2, 2021 August 2, 2021 August 2, 2021Dokument1 SeiteCBC Test Name Result Result Result Result Reference Range August 21, 2021 August 2, 2021 August 2, 2021 August 2, 2021jpmNoch keine Bewertungen
- Automatic Haematology AnalyzerDokument56 SeitenAutomatic Haematology AnalyzerIndah100% (1)
- Fluid Therapy (Ali Haedar)Dokument25 SeitenFluid Therapy (Ali Haedar)Atika LuqyanaNoch keine Bewertungen
- 2022 - 11 - 13 NAmigoDokument57 Seiten2022 - 11 - 13 NAmigoNuria AmigoNoch keine Bewertungen
- Relay Settings - XlsxsDokument18 SeitenRelay Settings - XlsxsAvinash KumarNoch keine Bewertungen
- Hematology Report: Test Result Ref - Range UnitDokument1 SeiteHematology Report: Test Result Ref - Range Unitmicklemagdy50Noch keine Bewertungen
- ATC Criticas+apresentaçåo Cópia CópiaDokument34 SeitenATC Criticas+apresentaçåo Cópia Cópiajramires37566100% (3)
- Carpentier Mitral Valve Regurgitation ClasifDokument45 SeitenCarpentier Mitral Valve Regurgitation ClasifKudor Szabadi Zoltán100% (1)
- Histogram InterpretationDokument34 SeitenHistogram InterpretationSagar Chandrakant Mhetre100% (4)
- b0907 FluidDokument43 Seitenb0907 FluidyamtotlNoch keine Bewertungen
- Acquired Aplastic Anemia: G7: Barrios, David, EsmileDokument14 SeitenAcquired Aplastic Anemia: G7: Barrios, David, EsmileAndrew Arnold David VillanuevaNoch keine Bewertungen
- 2003 ÀåÀ È PDFDokument33 Seiten2003 ÀåÀ È PDFCon Chồn Phép ThuậtNoch keine Bewertungen
- Biliary Stricture in Post LDLT RecipientDokument15 SeitenBiliary Stricture in Post LDLT Recipientchawlay.phyu87Noch keine Bewertungen
- Template LaboratoriumDokument78 SeitenTemplate Laboratoriumyani sutriyaniNoch keine Bewertungen
- Measurement of Blood Cells and Related ParametersDokument33 SeitenMeasurement of Blood Cells and Related ParametersKusuma P SitorusNoch keine Bewertungen
- IV Fluids and Electrolyte PhysiologyDokument64 SeitenIV Fluids and Electrolyte PhysiologypaulaNoch keine Bewertungen
- PerfusionDokument32 SeitenPerfusionRamisha RaidaNoch keine Bewertungen
- I. Demographic DataDokument3 SeitenI. Demographic DataBorge BalasaNoch keine Bewertungen
- SYOK - Desi Surya IniDokument40 SeitenSYOK - Desi Surya IniDesi Suryani DewiNoch keine Bewertungen
- Active Passive Capture2017 ClassslidesDokument37 SeitenActive Passive Capture2017 Classslidesᴛᴀɴᴍᴀy ᴋᴀʀᴀɴɢᴜᴛᴋᴀʀNoch keine Bewertungen
- Cardiac Muscle: Group 7 Saskia Nabilah Rania Sulviani Tasya Rafifah Danty MilleniaDokument19 SeitenCardiac Muscle: Group 7 Saskia Nabilah Rania Sulviani Tasya Rafifah Danty MilleniaRania SulvianiNoch keine Bewertungen
- Elektor Book 75Dokument113 SeitenElektor Book 75robertotoro2014Noch keine Bewertungen
- Pressure vs. Flow Essential Concepts PUC Ago 2019 V2 LTDokument78 SeitenPressure vs. Flow Essential Concepts PUC Ago 2019 V2 LTCristóbal Miño MoralesNoch keine Bewertungen
- Address: 100 International Blvd. Toronto, Ontario Canada M9W 6J6 Telephone: (877) 849-3637 Toll Free: (877) 849-3637 Fax: (905) 795-9891Dokument2 SeitenAddress: 100 International Blvd. Toronto, Ontario Canada M9W 6J6 Telephone: (877) 849-3637 Toll Free: (877) 849-3637 Fax: (905) 795-9891Adam SalihNoch keine Bewertungen
- Tickler Final PDFDokument29 SeitenTickler Final PDFSerious LeoNoch keine Bewertungen
- Hamda Mohammad Sa'adeh - PCI Final ReportDokument4 SeitenHamda Mohammad Sa'adeh - PCI Final Reportshamaamo19Noch keine Bewertungen
- Cardiac Muscle: Group 7 Saskia Nabilah Rania Sulviani Tasya Rafifah Danty MilleniaDokument18 SeitenCardiac Muscle: Group 7 Saskia Nabilah Rania Sulviani Tasya Rafifah Danty MilleniaRania SulvianiNoch keine Bewertungen
- DR - Sabah Noori 1Dokument26 SeitenDR - Sabah Noori 1Mighty AbodyNoch keine Bewertungen
- Arrythmia by AbnetDokument509 SeitenArrythmia by AbnetAbnet WondimuNoch keine Bewertungen
- LCMS Consumables Brochure NovDec 2022Dokument10 SeitenLCMS Consumables Brochure NovDec 2022Diego BermudezNoch keine Bewertungen
- Cardiovascular Physiology: by Dr. T.R. Ramachandran Professor Mahsa 07 June 2016Dokument40 SeitenCardiovascular Physiology: by Dr. T.R. Ramachandran Professor Mahsa 07 June 2016PATHMAPRIYA GANESANNoch keine Bewertungen
- Department of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungDokument61 SeitenDepartment of Cardiology and Vascular Medicine, Padjadjaran University School of Medicine Hasan Sadikin Hospital BandungMuhammad AmrieNoch keine Bewertungen
- Interpretation of HistogramDokument92 SeitenInterpretation of HistogramJagu ShahNoch keine Bewertungen
- AmrullahDokument69 SeitenAmrullahJunaedi YundingNoch keine Bewertungen
- New Standrd Rate (Folio) PDFDokument226 SeitenNew Standrd Rate (Folio) PDFJE MtceNoch keine Bewertungen
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDokument90 SeitenECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNoch keine Bewertungen
- Apheresis PrincipleDokument68 SeitenApheresis Principlemelisa asibalNoch keine Bewertungen
- Ficha Tecnica MOTOR BALDORDokument11 SeitenFicha Tecnica MOTOR BALDORcarlos.castillo.ing.1Noch keine Bewertungen
- Mail Order Form: Please Fill-In The Information Below COMPLETELYDokument1 SeiteMail Order Form: Please Fill-In The Information Below COMPLETELYtasarimkutusuNoch keine Bewertungen
- Liver Transplant Handbook Contents Introduction 1. Liver Liver Disease 2.Dokument31 SeitenLiver Transplant Handbook Contents Introduction 1. Liver Liver Disease 2.tasarimkutusuNoch keine Bewertungen
- The Emergence of Liver Transplantation For Hilar CholangiocarcinomaDokument109 SeitenThe Emergence of Liver Transplantation For Hilar CholangiocarcinomatasarimkutusuNoch keine Bewertungen
- Fulminant Hepatic Failure and Liver TransplantationDokument104 SeitenFulminant Hepatic Failure and Liver TransplantationtasarimkutusuNoch keine Bewertungen
- For Hepatocellular Carcinoma: Living Donor Liver TransplantationDokument46 SeitenFor Hepatocellular Carcinoma: Living Donor Liver TransplantationtasarimkutusuNoch keine Bewertungen
- Prevention of Recurrent Hepatitis B After Liver TransplantationDokument45 SeitenPrevention of Recurrent Hepatitis B After Liver TransplantationtasarimkutusuNoch keine Bewertungen
- Chorionic Bump in First-Trimester Sonography: SciencedirectDokument6 SeitenChorionic Bump in First-Trimester Sonography: SciencedirectEdward EdwardNoch keine Bewertungen
- What Is Multiple MyelomaDokument2 SeitenWhat Is Multiple MyelomaRegine Garcia Lagazo100% (1)
- Tolbert Medical Clinic Anniston, Alabama: Planning Assessment, Space Program & Site Test Fit AnalysisDokument15 SeitenTolbert Medical Clinic Anniston, Alabama: Planning Assessment, Space Program & Site Test Fit Analysisalassadi09Noch keine Bewertungen
- Resume PortfolioDokument1 SeiteResume Portfolioapi-491272428Noch keine Bewertungen
- SialolithiasisDokument38 SeitenSialolithiasismutiaaulianyNoch keine Bewertungen
- Medsave - Claim Form For MediclaimDokument1 SeiteMedsave - Claim Form For Mediclaimpawan1501Noch keine Bewertungen
- What Is Doctor of Physical TherapyDokument7 SeitenWhat Is Doctor of Physical TherapyDebra NajiNoch keine Bewertungen
- Statistics of National Morbidity and MortalityDokument30 SeitenStatistics of National Morbidity and MortalityKrystel Mae GarciaNoch keine Bewertungen
- Toc PDFDokument12 SeitenToc PDFraviraja moduguNoch keine Bewertungen
- Tramadol, Ketorolac, EterocoxibDokument4 SeitenTramadol, Ketorolac, EterocoxibEric de JulianNoch keine Bewertungen
- Resume For LPNDokument8 SeitenResume For LPNafllwwtjo100% (1)
- Flowchart For Assessing Illness in The Absence of The School NurseDokument1 SeiteFlowchart For Assessing Illness in The Absence of The School NurserahkelpNoch keine Bewertungen
- Team Code 34 PDokument22 SeitenTeam Code 34 PShivam TiwaryNoch keine Bewertungen
- English 10 Page EssayDokument13 SeitenEnglish 10 Page Essayapi-549614851Noch keine Bewertungen
- Learners and Safety and Emergency CardDokument6 SeitenLearners and Safety and Emergency CardAsielyn SamsonNoch keine Bewertungen
- Dr. Jigar PatelDokument6 SeitenDr. Jigar PatelJigar PatelNoch keine Bewertungen
- Pathophysiology of Acute GastroenteritisDokument5 SeitenPathophysiology of Acute Gastroenteritisheron_bayanin_15Noch keine Bewertungen
- Library Genesis PDFDokument8 SeitenLibrary Genesis PDFSipra PaulNoch keine Bewertungen
- Mds - Curriculum (Hust) Tongji Medical CollegeDokument45 SeitenMds - Curriculum (Hust) Tongji Medical CollegeMukunda RegmiNoch keine Bewertungen
- Introduction To Pathology Infectious DiseasesDokument37 SeitenIntroduction To Pathology Infectious DiseasesNirav PatelNoch keine Bewertungen
- WA Health Consent To Treatment Policy: Better Health Better Care Better ValueDokument42 SeitenWA Health Consent To Treatment Policy: Better Health Better Care Better ValueprabhaNoch keine Bewertungen
- PhysioEx Exercise 7 Activity 1Dokument6 SeitenPhysioEx Exercise 7 Activity 1Jorge CuevaNoch keine Bewertungen
- Introduction of Physical MedicineDokument39 SeitenIntroduction of Physical MedicineDrMd Nurul Hoque MiahNoch keine Bewertungen
- Ebook Berry Kohns Operating Room Technique 14Th Edition PDF Full Chapter PDFDokument67 SeitenEbook Berry Kohns Operating Room Technique 14Th Edition PDF Full Chapter PDFgerald.wesolowski623100% (22)
- Topic:: Relationship Between Theory and The Science and Practice of NursingDokument6 SeitenTopic:: Relationship Between Theory and The Science and Practice of NursingAhmad anasNoch keine Bewertungen
- Abnormal Uterine Bleeding in Reproductive-Age Women - Terminology and PALM-COEIN Etiology Classification - UpToDateDokument46 SeitenAbnormal Uterine Bleeding in Reproductive-Age Women - Terminology and PALM-COEIN Etiology Classification - UpToDateCristinaCaprosNoch keine Bewertungen
- Curriculum Vitae Indonesia International (Bio) Medical Students' Congress (INAMSC) 2019Dokument2 SeitenCurriculum Vitae Indonesia International (Bio) Medical Students' Congress (INAMSC) 2019bastomyNoch keine Bewertungen
- Clinicians Guide To Assessing and Counseling Older Drivers Sep 2020Dokument282 SeitenClinicians Guide To Assessing and Counseling Older Drivers Sep 2020lucia.oliveiraNoch keine Bewertungen
- Musculoskeletal Curriculum: History & Physical Exam of The ShoulderDokument60 SeitenMusculoskeletal Curriculum: History & Physical Exam of The Shoulderhis.thunder122100% (1)
- Albumin: Pathophysiologic Basis of Its Role in The Treatment of Cirrhosis and Its ComplicationsDokument26 SeitenAlbumin: Pathophysiologic Basis of Its Role in The Treatment of Cirrhosis and Its Complicationsravi rajNoch keine Bewertungen