Das könnte Ihnen auch gefallen
- Borderline Personality Disorder: The ultimate guide to borderline personality disorder including signs and symptoms, diagnosis, treatment, and how to improve and manage it!Von EverandBorderline Personality Disorder: The ultimate guide to borderline personality disorder including signs and symptoms, diagnosis, treatment, and how to improve and manage it!Noch keine Bewertungen
- Childhood Depression Presentation OutlineDokument7 SeitenChildhood Depression Presentation Outlineapi-290018716Noch keine Bewertungen
- E.2 Bipolar PPT 2017Dokument42 SeitenE.2 Bipolar PPT 2017Ptrc Lbr LpNoch keine Bewertungen
- Psychosocial Assessment of Older AdultsDokument42 SeitenPsychosocial Assessment of Older AdultsMarianne PradoNoch keine Bewertungen
- Anxiety Disorders in Children and Adolescent presentationCAPDokument59 SeitenAnxiety Disorders in Children and Adolescent presentationCAPAbelNoch keine Bewertungen
- Major Depression in Children and Adolescents: ObjectiveDokument2 SeitenMajor Depression in Children and Adolescents: ObjectiveJonty ArputhemNoch keine Bewertungen
- Depression in Children and Adolescents: Adapted by Julie ChiltonDokument38 SeitenDepression in Children and Adolescents: Adapted by Julie ChiltonGwendolyn PansoyNoch keine Bewertungen
- SEMINAR On DepressionDokument27 SeitenSEMINAR On Depressionlumina.sNoch keine Bewertungen
- Childhood Abuse, TraumaDokument44 SeitenChildhood Abuse, TraumaasoulNoch keine Bewertungen
- Personality DisordersDokument65 SeitenPersonality DisorderssherifNoch keine Bewertungen
- Depression Touro College of Undergraduate PsychologyDokument7 SeitenDepression Touro College of Undergraduate PsychologyErickNoch keine Bewertungen
- Psychologists Clinical Psychology American Psychological AssociationDokument12 SeitenPsychologists Clinical Psychology American Psychological AssociationrenivakunNoch keine Bewertungen
- Psychiatric Disorders in Childhood and AdolescenceDokument81 SeitenPsychiatric Disorders in Childhood and Adolescenceabriham100% (1)
- Mentalhealth 170225073540Dokument31 SeitenMentalhealth 170225073540Roginee Del SolNoch keine Bewertungen
- F.3. OCD Powerpoint 20161Dokument30 SeitenF.3. OCD Powerpoint 20161Ptrc Lbr Lp100% (1)
- Adolescent Problem - DepressionDokument27 SeitenAdolescent Problem - DepressionMeera AnnNoch keine Bewertungen
- Unit-4 Mental and Behavioral ProblemsDokument20 SeitenUnit-4 Mental and Behavioral ProblemsZain Ul abidinNoch keine Bewertungen
- Depressive DisordersDokument51 SeitenDepressive DisordersGiorgi TamazashviliNoch keine Bewertungen
- F.1 Anxiety 2016 PowePointDokument25 SeitenF.1 Anxiety 2016 PowePointPtrc Lbr LpNoch keine Bewertungen
- E.2 Bipolar PPT 2017Dokument42 SeitenE.2 Bipolar PPT 2017abrihamNoch keine Bewertungen
- Idcc Rachel State, MD/MPH Pgy 4 (10/15/12)Dokument24 SeitenIdcc Rachel State, MD/MPH Pgy 4 (10/15/12)Emily EresumaNoch keine Bewertungen
- Causes of Depression in TeenagersDokument4 SeitenCauses of Depression in TeenagerskreamerNoch keine Bewertungen
- Mood Disord Ers: DO, RN, MA NDokument39 SeitenMood Disord Ers: DO, RN, MA NKrishna BalsarzaNoch keine Bewertungen
- Activity 10 Day 2Dokument7 SeitenActivity 10 Day 2Crisha Ann Billones BacutaNoch keine Bewertungen
- G Mood Disorders MWDokument59 SeitenG Mood Disorders MWBehar AbdurahemanNoch keine Bewertungen
- Schizophrenia Spectrum and Other Psychotic DisordersDokument84 SeitenSchizophrenia Spectrum and Other Psychotic DisordersJara YumiNoch keine Bewertungen
- Basic Management of Juvenile Mood Disorders: Jeffrey I. Hunt, MDDokument46 SeitenBasic Management of Juvenile Mood Disorders: Jeffrey I. Hunt, MDzainiNoch keine Bewertungen
- PPD Ray 102307nnDokument51 SeitenPPD Ray 102307nnFatima AzzahraNoch keine Bewertungen
- A Parentsmedguide PDFDokument15 SeitenA Parentsmedguide PDFMikitaTorresNoch keine Bewertungen
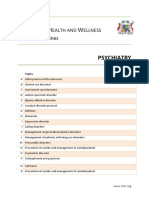
- PsychiatryDokument128 SeitenPsychiatrysumayyah hosanyNoch keine Bewertungen
- E.1 Depression PowerPoint 20151Dokument38 SeitenE.1 Depression PowerPoint 20151Ptrc Lbr LpNoch keine Bewertungen
- Psychiatric Disorders in Childhood and AdolescenceDokument81 SeitenPsychiatric Disorders in Childhood and AdolescenceDhartie FweshBoy NasifNoch keine Bewertungen
- E.3 DMDD 2017Dokument17 SeitenE.3 DMDD 2017Maria Helena Pedraza MNoch keine Bewertungen
- Impulse, Conduct and Disruptive Behaviour DisordersDokument46 SeitenImpulse, Conduct and Disruptive Behaviour DisordersManisha100% (4)
- Rushi MSCDokument33 SeitenRushi MSCRushikesh Jadhav0% (1)
- Rawatan Klien Dua DiagnosisDokument60 SeitenRawatan Klien Dua DiagnosisPUSAT LATIHAN AADKNoch keine Bewertungen
- Nursing Children and Adolescents With Bipolar Disorder: Assessment, Diagnosis, Treatment, and ManagementDokument8 SeitenNursing Children and Adolescents With Bipolar Disorder: Assessment, Diagnosis, Treatment, and ManagementmeronayezabuNoch keine Bewertungen
- Child Psychiatric DisordersDokument9 SeitenChild Psychiatric DisordersMonika JosephNoch keine Bewertungen
- The Impact of Depression Among Students in Iplc Senior High School-1Dokument3 SeitenThe Impact of Depression Among Students in Iplc Senior High School-1Roxanne TongcuaNoch keine Bewertungen
- Rawatan Klien Dua DiagnosisDokument62 SeitenRawatan Klien Dua DiagnosisPUSAT LATIHAN AADKNoch keine Bewertungen
- Confused Too Stressed OutDokument82 SeitenConfused Too Stressed OuttzichiNoch keine Bewertungen
- Mental Illness and Mental HealthDokument3 SeitenMental Illness and Mental HealthHarshad ParmarNoch keine Bewertungen
- Diagnosis of Mental IllnessDokument66 SeitenDiagnosis of Mental IllnessJorn Arvi ReyesNoch keine Bewertungen
- Borderline Personality Disorder 508Dokument21 SeitenBorderline Personality Disorder 508IntellibrainNoch keine Bewertungen
- Depression PP FVDokument62 SeitenDepression PP FVSharmela Brijmohan100% (1)
- New Anxiety For Med Rehab'OTDokument18 SeitenNew Anxiety For Med Rehab'OTEmmanuel AbiolaNoch keine Bewertungen
- Bipolar Disorder: Kim Carter Appalachian State UniversityDokument46 SeitenBipolar Disorder: Kim Carter Appalachian State UniversitySarangNoch keine Bewertungen
- Psyc 302 Week 10 Childhood AgingDokument54 SeitenPsyc 302 Week 10 Childhood AgingENoch keine Bewertungen
- DepressionDokument5 SeitenDepressionapi-336702702Noch keine Bewertungen
- Depression: WWW - Changethatmatters.Umn - EduDokument67 SeitenDepression: WWW - Changethatmatters.Umn - EduanushkaNoch keine Bewertungen
- Depression and Anxiety Concept MapDokument4 SeitenDepression and Anxiety Concept Mapsammillepointer86Noch keine Bewertungen
- Formulation and The Biopsychosocial Model Introduction For Psychiatry ResidentsDokument10 SeitenFormulation and The Biopsychosocial Model Introduction For Psychiatry ResidentsLennard Ashley Salaysay100% (5)
- Mood DisordersDokument14 SeitenMood DisordersHayat AL AKOUMNoch keine Bewertungen
- Aging and Mental HealthDokument77 SeitenAging and Mental HealthDarla SaulerNoch keine Bewertungen
- Depression: Nkondo Primary School-East Province RwandaDokument13 SeitenDepression: Nkondo Primary School-East Province RwandaKABERA RENENoch keine Bewertungen
- Mental HealthDokument96 SeitenMental HealthTinaHo100% (4)
- F.1 Anxiety 2016 PowePointDokument26 SeitenF.1 Anxiety 2016 PowePointKibru le EyesusNoch keine Bewertungen
- Coping with Bipolar Disorder: A CBT-Informed Guide to Living with Manic DepressionVon EverandCoping with Bipolar Disorder: A CBT-Informed Guide to Living with Manic DepressionNoch keine Bewertungen
- A Layperson's Guide to Living with Mental DiseaseVon EverandA Layperson's Guide to Living with Mental DiseaseNoch keine Bewertungen
- Energy Crisis of PakistanDokument4 SeitenEnergy Crisis of PakistannarmeennasirNoch keine Bewertungen
- Css Time Table 2014 PDFDokument1 SeiteCss Time Table 2014 PDFk_Dashy8465Noch keine Bewertungen
- Crux of Pak-China RelationsDokument4 SeitenCrux of Pak-China RelationsnarmeennasirNoch keine Bewertungen
- Arab Spring & Pakistan PDFDokument2 SeitenArab Spring & Pakistan PDFZaheer Ahmed TanoliNoch keine Bewertungen
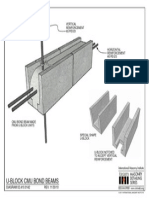
- U-Block Cmu Bond Beams: Vertical Reinforcement As Req'DDokument1 SeiteU-Block Cmu Bond Beams: Vertical Reinforcement As Req'DnarmeennasirNoch keine Bewertungen
- Auto Cad Title BlocksDokument11 SeitenAuto Cad Title Blocksmohammed abdul sami munwer100% (1)
- 2009-12 - McCauley - Depressive Disorders in Children and AdolescentsDokument52 Seiten2009-12 - McCauley - Depressive Disorders in Children and AdolescentsnarmeennasirNoch keine Bewertungen
- Latino Parent StudyDokument17 SeitenLatino Parent StudyLatino USANoch keine Bewertungen
- RRL (Local Literature)Dokument5 SeitenRRL (Local Literature)clarissamay33Noch keine Bewertungen
- Practical Research 2 - Causes of DepressionDokument7 SeitenPractical Research 2 - Causes of DepressionPrincess BuenosairesNoch keine Bewertungen
- Psychoanalytic Theories: Carl Jung (1875-1961)Dokument6 SeitenPsychoanalytic Theories: Carl Jung (1875-1961)Sean KingNoch keine Bewertungen
- Effects of COVID-19 On Children's Mental HealthDokument21 SeitenEffects of COVID-19 On Children's Mental Healthduwa douglasNoch keine Bewertungen
- Sleiman SemaanDokument67 SeitenSleiman SemaanJean-Paul Moubarak100% (1)
- Map 510 Capstone Reflection - RJ MontesDokument7 SeitenMap 510 Capstone Reflection - RJ Montesapi-635328971Noch keine Bewertungen
- The Significance of Choral SingingDokument18 SeitenThe Significance of Choral SingingprisconetrunnerNoch keine Bewertungen
- List of Mental Rubrics in HomeopathyDokument23 SeitenList of Mental Rubrics in Homeopathyatuguesp88% (25)
- Bully PDFDokument6 SeitenBully PDFNSNoch keine Bewertungen
- 2020 NGSC Mission Team 18 MagazineDokument10 Seiten2020 NGSC Mission Team 18 MagazineIbu OluyiNoch keine Bewertungen
- Mental HealthDokument17 SeitenMental HealthstreetkeykNoch keine Bewertungen
- Revised Children's Anxiety and Depression Scale (And Subscales) (Rcads)Dokument6 SeitenRevised Children's Anxiety and Depression Scale (And Subscales) (Rcads)e_nov78Noch keine Bewertungen
- The Impact of Using Drugs, Misuse, and Abuse Mapeh9 Lesson-Exemplar-HealthDokument5 SeitenThe Impact of Using Drugs, Misuse, and Abuse Mapeh9 Lesson-Exemplar-HealthKrishia Ich MagpileNoch keine Bewertungen
- 5 A Comprehensive Meta-Analysis of Interpretation Biases in DepressionDokument16 Seiten5 A Comprehensive Meta-Analysis of Interpretation Biases in DepressionАлексейNoch keine Bewertungen
- Libia Hernandez-Martinez - Capstone Paper Final DraftDokument4 SeitenLibia Hernandez-Martinez - Capstone Paper Final Draftapi-606444823Noch keine Bewertungen
- Circus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressDokument151 SeitenCircus Psychology An Applied Guide To Thriving Under The Big Top 2022018105 2022018106 9781032266343 9781032266435 9781003289227 - CompressLaura GăvanNoch keine Bewertungen
- Anxiolytics and AntidepressantsDokument271 SeitenAnxiolytics and AntidepressantsAmir PeljtoNoch keine Bewertungen
- Assignment 2. PSYC6163 Jennifer JosephDokument7 SeitenAssignment 2. PSYC6163 Jennifer JosephUrvashi Mendpara100% (3)
- Becks Depression IndexDokument2 SeitenBecks Depression IndexChukwuemeka AghasiliNoch keine Bewertungen
- 2 Qi WQufx 4 X 1 El 9 LKUDr LDokument4 Seiten2 Qi WQufx 4 X 1 El 9 LKUDr LSatish BohatNoch keine Bewertungen
- Benefits of TherapyDokument4 SeitenBenefits of Therapymr perfectNoch keine Bewertungen
- Concept PaperDokument11 SeitenConcept PaperSun ShineNoch keine Bewertungen
- The Impact of Social Isolation and Cognitive Decline in Older AduDokument31 SeitenThe Impact of Social Isolation and Cognitive Decline in Older Adumadalena limaNoch keine Bewertungen
- 2017 - Zinosal y Riesgo de Suicidio - NobileDokument4 Seiten2017 - Zinosal y Riesgo de Suicidio - NobileNicolás BNoch keine Bewertungen
- 2017-Review of Prenatal Maternal Mental Health and The Development of Infant TemperamentDokument13 Seiten2017-Review of Prenatal Maternal Mental Health and The Development of Infant TemperamentbleuegirlmxNoch keine Bewertungen
- Stress Levels Caused by Learning During Covid-19 Readjustment in Adolescents in Thailand and The SolutionDokument8 SeitenStress Levels Caused by Learning During Covid-19 Readjustment in Adolescents in Thailand and The SolutionIJAR JOURNALNoch keine Bewertungen
- Mood Disorders Lesson PlanDokument17 SeitenMood Disorders Lesson Planapi-2841042060% (1)
- Psychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Dokument53 SeitenPsychological Testing-II Report Submitted by Fatima Syed Fa17-Bpy-016Fatima SyedNoch keine Bewertungen
- I. Ecologic Model A. HypothesisDokument5 SeitenI. Ecologic Model A. HypothesisTintin LevidaNoch keine Bewertungen