Das könnte Ihnen auch gefallen
- Decisions and Consequences: The Realities of Being a ManVon EverandDecisions and Consequences: The Realities of Being a ManNoch keine Bewertungen
- Acute AgitationDokument83 SeitenAcute AgitationSamuel FikaduNoch keine Bewertungen
- Multiple Sclerosis, A Simple Guide To The Condition, Treatment And Related ConditionsVon EverandMultiple Sclerosis, A Simple Guide To The Condition, Treatment And Related ConditionsNoch keine Bewertungen
- Forced Normalization - Clinical and Therapeutic RelevanceDokument8 SeitenForced Normalization - Clinical and Therapeutic Relevancejuan_bacha_1Noch keine Bewertungen
- Pathy's Principles and Practice of Geriatric MedicineVon EverandPathy's Principles and Practice of Geriatric MedicineAlan J. SinclairNoch keine Bewertungen
- Adolescent DepressionDokument26 SeitenAdolescent DepressionRajakkad ANoch keine Bewertungen
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenVon EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNoch keine Bewertungen
- Psychosomatic in Psychiatry - UNTAD 2012Dokument18 SeitenPsychosomatic in Psychiatry - UNTAD 2012Fadjarr WahidNoch keine Bewertungen
- Pseudoseizures and Dissociative DisordersDokument5 SeitenPseudoseizures and Dissociative DisordersLaura AndreiNoch keine Bewertungen
- Ganser SyndromeDokument3 SeitenGanser Syndromesomebody_maNoch keine Bewertungen
- Childhood Depression Presentation OutlineDokument7 SeitenChildhood Depression Presentation Outlineapi-290018716Noch keine Bewertungen
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDokument62 SeitenAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2Noch keine Bewertungen
- General Questions (Mood Disorder)Dokument5 SeitenGeneral Questions (Mood Disorder)Zubair MushtaqNoch keine Bewertungen
- PPDGJ 3 PDFDokument279 SeitenPPDGJ 3 PDFtri ummiNoch keine Bewertungen
- Types of DepressionDokument12 SeitenTypes of DepressionKADAMBARINoch keine Bewertungen
- (2017) Delirium. Primary Care - Clinics in Office PracticeDokument19 Seiten(2017) Delirium. Primary Care - Clinics in Office PracticeDavid Morales ZepedaNoch keine Bewertungen
- Traumatic Brain InjuryDokument17 SeitenTraumatic Brain InjuryRori de los ReyesNoch keine Bewertungen
- Neurocognitive DisordersDokument31 SeitenNeurocognitive DisordersMonina JonesNoch keine Bewertungen
- Podcast Anxiety and DepressionDokument5 SeitenPodcast Anxiety and DepressionSyifa Olyfiani SariNoch keine Bewertungen
- Depression Children PDFDokument2 SeitenDepression Children PDFConstanzaNoch keine Bewertungen
- Addiction, Dependence, and ToleranceDokument26 SeitenAddiction, Dependence, and ToleranceCarter A KellyNoch keine Bewertungen
- Mental Disorders: Sub Ject: Clinical Psychology Presented By: PHD - Mariana CernitanuDokument34 SeitenMental Disorders: Sub Ject: Clinical Psychology Presented By: PHD - Mariana CernitanuAlbert PruteanuNoch keine Bewertungen
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDokument20 SeitenPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Noch keine Bewertungen
- Depression in Older PeopleDokument4 SeitenDepression in Older PeopleAlina AlinaNoch keine Bewertungen
- Psy 105 Neurological DisordersDokument11 SeitenPsy 105 Neurological Disordersdesiree leornasNoch keine Bewertungen
- Mind Body Link PDFDokument12 SeitenMind Body Link PDFProf Dr Kathirrvelu SubramanianNoch keine Bewertungen
- Cognitive Rehabilitation in SchizophreniaDokument12 SeitenCognitive Rehabilitation in SchizophreniaSanthosh ReddyNoch keine Bewertungen
- Malingering NbiDokument5 SeitenMalingering NbiPridina SyadirahNoch keine Bewertungen
- Role of Vitamin D in Schizophrenia in Elderly PatientDokument3 SeitenRole of Vitamin D in Schizophrenia in Elderly PatientJAVED ATHER SIDDIQUINoch keine Bewertungen
- BPSD GuidelineDokument16 SeitenBPSD GuidelineJohan DjongiantoNoch keine Bewertungen
- Anxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDDokument38 SeitenAnxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDadystiNoch keine Bewertungen
- Introduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPDokument33 SeitenIntroduction To Psychiatric Nursing: Mercedes A Perez-Millan MSN, ARNPSachiko Yosores100% (1)
- Notes On PsychiatryDokument10 SeitenNotes On PsychiatryMark VillenaNoch keine Bewertungen
- Cognitive Rehab 101 Webinar Handout 051817Dokument36 SeitenCognitive Rehab 101 Webinar Handout 051817klockNoch keine Bewertungen
- Traumatic Brain InjuryDokument14 SeitenTraumatic Brain InjuryBelle CaharopNoch keine Bewertungen
- Chapter 23 - Medication Interest ModelDokument83 SeitenChapter 23 - Medication Interest ModelNaomi LiangNoch keine Bewertungen
- Degenerative Diseases of The Brain 2Dokument66 SeitenDegenerative Diseases of The Brain 2Janie-Vi Villamor Ismael-GorospeNoch keine Bewertungen
- What's NextDokument27 SeitenWhat's NextBethany House PublishersNoch keine Bewertungen
- Stress and Personality DDokument7 SeitenStress and Personality DAdriana NegrescuNoch keine Bewertungen
- Vitamins, Supplements, Herbal Medicines, and ArrhythmiasDokument12 SeitenVitamins, Supplements, Herbal Medicines, and ArrhythmiashyntnenNoch keine Bewertungen
- M S eDokument87 SeitenM S eabhishek agarwalNoch keine Bewertungen
- Postconcussive Syndrome (PCS) Clinical Practice Guideline: Occupational TherapyDokument7 SeitenPostconcussive Syndrome (PCS) Clinical Practice Guideline: Occupational TherapyNicoleta Stoica100% (1)
- Schizophrenia: National Institute of Mental HealthDokument8 SeitenSchizophrenia: National Institute of Mental HealthCristian ZuñigaNoch keine Bewertungen
- Traumatic Stress - Effects On The Brain PDFDokument17 SeitenTraumatic Stress - Effects On The Brain PDFDaniel Londoño GuzmánNoch keine Bewertungen
- Degenerative Neurologic DisordersDokument29 SeitenDegenerative Neurologic DisordersVIDYANoch keine Bewertungen
- Schizoaffective - Disorder - FactsheetDokument9 SeitenSchizoaffective - Disorder - FactsheetGeraldVal100% (1)
- NppcityDokument63 SeitenNppcityMohammad JoharNoch keine Bewertungen
- Bipolar DepressionDokument5 SeitenBipolar DepressionRosalba GiovannelliNoch keine Bewertungen
- Schauss - A Critical Analysis of The Diet of Juvenile OffendersDokument21 SeitenSchauss - A Critical Analysis of The Diet of Juvenile OffenderslalipredebonNoch keine Bewertungen
- Neuroleptic Advers ReactionDokument65 SeitenNeuroleptic Advers Reactionayu yulianti100% (1)
- Disorders in Childhood and AdolescenceDokument6 SeitenDisorders in Childhood and AdolescenceCamille Joy BaliliNoch keine Bewertungen
- Psychiatric History & MSE: Bivin JB Department of Psychiatric Nursing Mar Baselios College of NursingDokument56 SeitenPsychiatric History & MSE: Bivin JB Department of Psychiatric Nursing Mar Baselios College of NursingHardeep KaurNoch keine Bewertungen
- What Happened To You Book Discussion Guide-National VersionDokument7 SeitenWhat Happened To You Book Discussion Guide-National Versionaulia normaNoch keine Bewertungen
- Assertive Community Treatment TreatmentOptions 2018Dokument2 SeitenAssertive Community Treatment TreatmentOptions 2018titik dyahNoch keine Bewertungen
- Individual Music Therapy For Depression: Randomised Controlled TrialDokument9 SeitenIndividual Music Therapy For Depression: Randomised Controlled TrialSarah HarahapNoch keine Bewertungen
- CATIE Trial Summary PaperDokument14 SeitenCATIE Trial Summary PaperNim RodNoch keine Bewertungen
- Psych Notes Case FilesDokument5 SeitenPsych Notes Case FilesMitz JuneNoch keine Bewertungen
- Somatoform Disorders 2019Dokument91 SeitenSomatoform Disorders 2019Poonam RanaNoch keine Bewertungen
- Psikogero B11Dokument90 SeitenPsikogero B11Eva Yeni RustianaNoch keine Bewertungen
- Recovering After A StrokeDokument17 SeitenRecovering After A StrokeTiffany MatthewsNoch keine Bewertungen
- Egas MonizDokument17 SeitenEgas Monizdrkadiyala2Noch keine Bewertungen
- Click Icon To Add PictureDokument52 SeitenClick Icon To Add Picturedrkadiyala2Noch keine Bewertungen
- Collective BehaviourDokument53 SeitenCollective Behaviourdrkadiyala2Noch keine Bewertungen
- Anesthesia For TurpDokument5 SeitenAnesthesia For Turpdrkadiyala2Noch keine Bewertungen
- Mental RetardationDokument37 SeitenMental Retardationdrkadiyala2100% (1)
- Panic Disorder With AgoraphobiaDokument55 SeitenPanic Disorder With Agoraphobiadrkadiyala2100% (2)
- Dissertation GuidelinesDokument9 SeitenDissertation Guidelinesrejipg86% (7)
- Addenbrooke's Cognitive Examination in TeluguDokument6 SeitenAddenbrooke's Cognitive Examination in Telugudrkadiyala250% (2)
- Fat EmbolismDokument26 SeitenFat Embolismdrkadiyala2Noch keine Bewertungen
- Ipde ScreeningDokument4 SeitenIpde Screeningdrkadiyala267% (3)
- Obsessive Compulsive Spectrum DisordersDokument62 SeitenObsessive Compulsive Spectrum Disordersdrkadiyala2Noch keine Bewertungen
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDokument62 SeitenAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2Noch keine Bewertungen
- DepressionDokument62 SeitenDepressiondrkadiyala2Noch keine Bewertungen
- Bipolar DepressionDokument81 SeitenBipolar Depressiondrkadiyala2Noch keine Bewertungen
- Lithium Clinical Uses & Adverse EffectsDokument75 SeitenLithium Clinical Uses & Adverse Effectsdrkadiyala2Noch keine Bewertungen
- Treatment Resistant OcdDokument70 SeitenTreatment Resistant Ocddrkadiyala2100% (1)
- CBT in ChildrenDokument39 SeitenCBT in Childrendrkadiyala2100% (1)
- Fat EmbolismDokument26 SeitenFat Embolismdrkadiyala2Noch keine Bewertungen
- Dialectical Behaviour TherapyDokument57 SeitenDialectical Behaviour Therapydrkadiyala2Noch keine Bewertungen
- Sensory Process and PerceptionDokument58 SeitenSensory Process and Perceptiondrkadiyala2Noch keine Bewertungen
- Panic Disorder - Etiology & Clinical FeaturesDokument49 SeitenPanic Disorder - Etiology & Clinical Featuresdrkadiyala2Noch keine Bewertungen
- Family TherapyDokument92 SeitenFamily Therapydrkadiyala2100% (1)
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDokument62 SeitenAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala267% (3)
- Obsessive Compulsive Spectrum DisordersDokument62 SeitenObsessive Compulsive Spectrum Disordersdrkadiyala2Noch keine Bewertungen
- Aetiology & Clinical Features of Alzheimers DiseaseDokument100 SeitenAetiology & Clinical Features of Alzheimers Diseasedrkadiyala2Noch keine Bewertungen
- Diagnosis, Assessment and Management of OCDDokument116 SeitenDiagnosis, Assessment and Management of OCDdrkadiyala2100% (2)
- DeliriumDokument72 SeitenDeliriumdrkadiyala2100% (2)
- Etiology of OCD: Chairperson: DR Anupama Presenter: DR ChandiniDokument35 SeitenEtiology of OCD: Chairperson: DR Anupama Presenter: DR Chandinidrkadiyala2Noch keine Bewertungen
- Vascular DementiaDokument57 SeitenVascular Dementiadrkadiyala2Noch keine Bewertungen
- Theories of LearningDokument76 SeitenTheories of Learningdrkadiyala2Noch keine Bewertungen
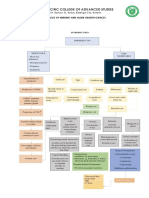
- CoE - Pathway Design Manual V15Dokument39 SeitenCoE - Pathway Design Manual V15AljoharaNoch keine Bewertungen
- HandbookHandbook of EvidenceBased Practices in Intellectual and Developmental Disabilities PDF of EvidenceBased Practices in Intellectual and Developmental DisabilitiesDokument1.005 SeitenHandbookHandbook of EvidenceBased Practices in Intellectual and Developmental Disabilities PDF of EvidenceBased Practices in Intellectual and Developmental DisabilitiesMihaela Neagu100% (11)
- DERMOID CYST FINAL NaDokument56 SeitenDERMOID CYST FINAL NaRhobic ManansalaNoch keine Bewertungen
- Somatization DisordersDokument26 SeitenSomatization DisordersAljohn GalangNoch keine Bewertungen
- Antipsychotics Pharm 3 Year 2Dokument19 SeitenAntipsychotics Pharm 3 Year 2Dua'a Al-HamdanNoch keine Bewertungen
- JCIA Handbook 2020Dokument61 SeitenJCIA Handbook 2020WAQASNoch keine Bewertungen
- Final Capstone PaperDokument15 SeitenFinal Capstone Paperapi-478784238Noch keine Bewertungen
- Animal HusbandryDokument69 SeitenAnimal HusbandryKabi RockNoch keine Bewertungen
- Why To Not Legalize EuthanasiaDokument5 SeitenWhy To Not Legalize EuthanasiaScotiaccap2016Noch keine Bewertungen
- Scid2 BPDDokument4 SeitenScid2 BPDRamonaStereaNoch keine Bewertungen
- Lesson Plan - Detecting The Mood Disorder FinalDokument2 SeitenLesson Plan - Detecting The Mood Disorder FinalTrixie MizonaNoch keine Bewertungen
- Panic DisorderDokument14 SeitenPanic DisorderMatthew MckenzieNoch keine Bewertungen
- Paediatrics III (A)Dokument1 SeitePaediatrics III (A)AlolikaNoch keine Bewertungen
- Clinical Practice Guidelines - 2017Dokument54 SeitenClinical Practice Guidelines - 2017Cem ÜnsalNoch keine Bewertungen
- Twenty Things To Know About Deep Brain Stimulation, 1E (2015) (PDF) (UnitedVRG)Dokument297 SeitenTwenty Things To Know About Deep Brain Stimulation, 1E (2015) (PDF) (UnitedVRG)amir11601Noch keine Bewertungen
- Community Health NursingDokument11 SeitenCommunity Health NursingJaylaiza Jane CaoileNoch keine Bewertungen
- Overtraining Syndrome (OTS) and Relative Energy Deficiency in Sport (RED S) : Shared Pathways, Symptoms and ComplexitiesDokument30 SeitenOvertraining Syndrome (OTS) and Relative Energy Deficiency in Sport (RED S) : Shared Pathways, Symptoms and ComplexitiesHugo TintiNoch keine Bewertungen
- Asperger's Syndrome in AdultsDokument7 SeitenAsperger's Syndrome in AdultsWillyOaksNoch keine Bewertungen
- OS Automotive Electromech L4Dokument76 SeitenOS Automotive Electromech L4Aida Mohammed80% (5)
- J Neurol Neurosurg Psychiatry 2008 Jankovic 368 76Dokument9 SeitenJ Neurol Neurosurg Psychiatry 2008 Jankovic 368 76Noven da LopezNoch keine Bewertungen
- Zhou 2020Dokument5 SeitenZhou 2020Daniel Ignacio Pérez ÁlvarezNoch keine Bewertungen
- Annual Progress in Child Psychiatry and Child Development 2000 2001 Annual Progress in Child Psychiatry and Child Development PDFDokument594 SeitenAnnual Progress in Child Psychiatry and Child Development 2000 2001 Annual Progress in Child Psychiatry and Child Development PDFRuxandra Gorbaciov100% (1)
- ProcDNA Claims Data Case Study SubmissionDokument2.210 SeitenProcDNA Claims Data Case Study SubmissionAtharva AnchalwarNoch keine Bewertungen
- This Is It NCD Case PresentationDokument31 SeitenThis Is It NCD Case PresentationEli BolusaNoch keine Bewertungen
- Non-Destructive Diagnostics of Concrete FloorsDokument158 SeitenNon-Destructive Diagnostics of Concrete Floorsmekkawi6650Noch keine Bewertungen
- Kecelaruan Mood: Profesor Dr. Kamarulzaman KamaruddinDokument19 SeitenKecelaruan Mood: Profesor Dr. Kamarulzaman KamaruddinbangarudaugtherNoch keine Bewertungen
- Early Diagnostic Markers For Neonatal Sepsis Comparing Procalcitonin (PCT) and C-Reactive Protein (CRP)Dokument5 SeitenEarly Diagnostic Markers For Neonatal Sepsis Comparing Procalcitonin (PCT) and C-Reactive Protein (CRP)IqbalNoch keine Bewertungen
- Personality in PsychologyDokument34 SeitenPersonality in PsychologyReader100% (1)
- Attending Physician Name: Medical Information Sheet - Medif - Part 2Dokument1 SeiteAttending Physician Name: Medical Information Sheet - Medif - Part 2San Ban CastroNoch keine Bewertungen
- Academic Study TemplateDokument35 SeitenAcademic Study TemplateAngel ShivayaNoch keine Bewertungen