Das könnte Ihnen auch gefallen
- Author Section Editor Deputy Editor Contributor DisclosuresDokument10 SeitenAuthor Section Editor Deputy Editor Contributor DisclosuresannisNoch keine Bewertungen
- Women's Imaging: MRI with Multimodality CorrelationVon EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownBewertung: 5 von 5 Sternen5/5 (1)
- Artifacts in Diagnostic Ultrasound: Grayscale ArtifactsVon EverandArtifacts in Diagnostic Ultrasound: Grayscale ArtifactsNoch keine Bewertungen
- ULTRASOUNDDokument14 SeitenULTRASOUNDpriyadharshini100% (1)
- Ultrasonography of The Hepatobiliary TractDokument9 SeitenUltrasonography of The Hepatobiliary TractPaola Méndez NeciosupNoch keine Bewertungen
- Mods of UltrasoundDokument22 SeitenMods of UltrasoundEnrique Valdez JordanNoch keine Bewertungen
- 2a JB Knobology 0Dokument63 Seiten2a JB Knobology 0Lorena ZaroniuNoch keine Bewertungen
- Vascular Ultrasound TrainingDokument5 SeitenVascular Ultrasound TrainingLyleHarris0% (1)
- Extrahepatic Biliary ObstructionDokument44 SeitenExtrahepatic Biliary ObstructionOssama Abd Al-amierNoch keine Bewertungen
- Bosniak ClassificationDokument19 SeitenBosniak ClassificationGirish Kumar100% (1)
- Abdominal UltrasonographyDokument3 SeitenAbdominal UltrasonographydokanadNoch keine Bewertungen
- Liquid Biopsy in Urogenital Cancers and its Clinical UtilityVon EverandLiquid Biopsy in Urogenital Cancers and its Clinical UtilitySeyed Mohammad Kazem AghamirNoch keine Bewertungen
- Classic Radiology SignsDokument9 SeitenClassic Radiology SignsJui DirDapNoch keine Bewertungen
- Contrast Media in Diagnostic RadiologyDokument56 SeitenContrast Media in Diagnostic RadiologyFaiq Syukri Bin SaparudinNoch keine Bewertungen
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsVon EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNoch keine Bewertungen
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDokument26 SeitenAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNoch keine Bewertungen
- Schwartz2002 PDFDokument7 SeitenSchwartz2002 PDFnova sorayaNoch keine Bewertungen
- Normal Variant in Abdominal UltrasounDokument20 SeitenNormal Variant in Abdominal Ultrasounshanks spearsonNoch keine Bewertungen
- UZVDokument56 SeitenUZVGoran MaliNoch keine Bewertungen
- Billiary SystemDokument60 SeitenBilliary SystemDONALD UNASHENoch keine Bewertungen
- 3 Abdominal Ultrasound Imaging AnatomyDokument7 Seiten3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarNoch keine Bewertungen
- Point of Care Ultrasound (Pocus) : Introduction: George A. FoxDokument76 SeitenPoint of Care Ultrasound (Pocus) : Introduction: George A. FoxAna Belen Viteri LuzuriagaNoch keine Bewertungen
- Short Hand Book of UltrasoundDokument106 SeitenShort Hand Book of Ultrasoundjnracquahxhamiel100% (2)
- Guidelines For Obstetric UltrasoundDokument10 SeitenGuidelines For Obstetric UltrasoundlittlefeNoch keine Bewertungen
- Ultrasound Made EasyDokument7 SeitenUltrasound Made EasyAnonymous ZUaUz1wwNoch keine Bewertungen
- Imaging Abdominal Trauma Focus On FAST Revisi DR - BahtiarDokument54 SeitenImaging Abdominal Trauma Focus On FAST Revisi DR - BahtiarJackson HakimNoch keine Bewertungen
- Doppler Ultrasound of The KidneysDokument23 SeitenDoppler Ultrasound of The KidneysivoklarinNoch keine Bewertungen
- Doppler Basics: DR - Priyatamjee BussaryDokument79 SeitenDoppler Basics: DR - Priyatamjee BussarydrsanndeepNoch keine Bewertungen
- Sonography PhysicsDokument42 SeitenSonography PhysicsAhmad AliNoch keine Bewertungen
- Ultrasound of Thyroid, Parathyroid Glands and Neck Lymph NodesDokument64 SeitenUltrasound of Thyroid, Parathyroid Glands and Neck Lymph Nodesnaga999100% (2)
- Radiology Notes - UltrasoundDokument15 SeitenRadiology Notes - UltrasoundborstNoch keine Bewertungen
- Principlesofdopplerultrasound 130514165605 Phpapp02Dokument92 SeitenPrinciplesofdopplerultrasound 130514165605 Phpapp02csngiu100% (2)
- Doppler Ultrasonography of The Lower Extremity ArteriesDokument34 SeitenDoppler Ultrasonography of The Lower Extremity ArteriesNidaa MubarakNoch keine Bewertungen
- Doppler UltrasoundDokument2 SeitenDoppler UltrasoundReiruki SawadaNoch keine Bewertungen
- MediastiniumDokument25 SeitenMediastiniumahmedzakaria0Noch keine Bewertungen
- Fluid Collection USGDokument103 SeitenFluid Collection USGhendrizalzubirNoch keine Bewertungen
- Advanced Topics in Biomedical EngineeringDokument35 SeitenAdvanced Topics in Biomedical EngineeringAmmer SaifullahNoch keine Bewertungen
- General UltrasoundDokument114 SeitenGeneral Ultrasoundgilbert centerNoch keine Bewertungen
- Doppler UltrasoundDokument12 SeitenDoppler UltrasoundMuhammad Shayan Farooq100% (1)
- Fetal Biometry and Growth: Callen'S Ultrasonography in Obstetrics and Gynecology (Sixth Edition)Dokument27 SeitenFetal Biometry and Growth: Callen'S Ultrasonography in Obstetrics and Gynecology (Sixth Edition)nellieauthorNoch keine Bewertungen
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyVon EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyNoch keine Bewertungen
- Cme Fast ScanDokument25 SeitenCme Fast Scannirmal raj100% (1)
- Ultrasound Evaluation of Renal Artery StenosisDokument24 SeitenUltrasound Evaluation of Renal Artery StenosisNguyen Tran CanhNoch keine Bewertungen
- Knee UltrasoundDokument6 SeitenKnee UltrasoundAndrei GianinaNoch keine Bewertungen
- AIUM Medical Ultrasound SafetyDokument60 SeitenAIUM Medical Ultrasound Safetyscuby660Noch keine Bewertungen
- Ultrasound and DopplerDokument22 SeitenUltrasound and Dopplerpri_292100% (1)
- Lecture 7 Doppler and HaemodynamicsDokument54 SeitenLecture 7 Doppler and HaemodynamicsattooNoch keine Bewertungen
- Very Common Questions:-: PhysiologyDokument15 SeitenVery Common Questions:-: PhysiologyJohn M. HemsworthNoch keine Bewertungen
- Pleural Puncture/thoracentesis: Pretty Laura ListianiDokument21 SeitenPleural Puncture/thoracentesis: Pretty Laura ListianirastaNoch keine Bewertungen
- Doppler of Varicose VeinsDokument85 SeitenDoppler of Varicose VeinsDiaa Eldeeb100% (2)
- Thyroid UltrasoundDokument62 SeitenThyroid Ultrasounddrmoscalin8774Noch keine Bewertungen
- Prostate Focused Ultrasound TherapyDokument17 SeitenProstate Focused Ultrasound TherapypuchioNoch keine Bewertungen
- Lower Extremity Venous Protocol 14Dokument3 SeitenLower Extremity Venous Protocol 14api-276847924Noch keine Bewertungen
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachVon EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriNoch keine Bewertungen
- Clinical PET/MRIVon EverandClinical PET/MRIOnofrio Antonio CatalanoNoch keine Bewertungen
- Skeletal TraumaDokument56 SeitenSkeletal Traumag1381821Noch keine Bewertungen
- Git LymphomasDokument43 SeitenGit Lymphomasg1381821Noch keine Bewertungen
- Thyroid MalignancyDokument65 SeitenThyroid Malignancyg1381821Noch keine Bewertungen
- Concepts of Radiologic ScienceDokument57 SeitenConcepts of Radiologic Scienceg1381821Noch keine Bewertungen
- Diffrential Diagnosis of Gastric Masses and NarrowingDokument62 SeitenDiffrential Diagnosis of Gastric Masses and Narrowingg1381821Noch keine Bewertungen
- Intestinal Obstruction in ChildrenDokument63 SeitenIntestinal Obstruction in Childreng1381821Noch keine Bewertungen
- Radiographic FILMDokument54 SeitenRadiographic FILMg1381821Noch keine Bewertungen
- The Urethra and Male Genital TractDokument70 SeitenThe Urethra and Male Genital Tractg1381821Noch keine Bewertungen
- Brain IschemiaDokument43 SeitenBrain Ischemiag1381821Noch keine Bewertungen
- Pulmonary HypertensionDokument43 SeitenPulmonary Hypertensiong1381821Noch keine Bewertungen
- Breast UltrasoundDokument46 SeitenBreast Ultrasoundg138182175% (4)
- Health PhysicsDokument33 SeitenHealth Physicsg1381821Noch keine Bewertungen
- Infant Cranial UltrasoundDokument73 SeitenInfant Cranial Ultrasoundg1381821100% (1)
- Case Presentation: Radiology HMCDokument78 SeitenCase Presentation: Radiology HMCg1381821Noch keine Bewertungen
- Excretory UrographyDokument64 SeitenExcretory Urographyg1381821Noch keine Bewertungen
- Medical Devices On The Chest X RayDokument114 SeitenMedical Devices On The Chest X Rayg1381821Noch keine Bewertungen
- Case Presentation: DR Tariq Masood TMO Radiology Department, HMCDokument82 SeitenCase Presentation: DR Tariq Masood TMO Radiology Department, HMCg1381821Noch keine Bewertungen
- Radiology Department Hayat Abad Medical ComplexDokument24 SeitenRadiology Department Hayat Abad Medical Complexg1381821Noch keine Bewertungen
- Paediatric Abdominal MassesDokument73 SeitenPaediatric Abdominal Massesg1381821Noch keine Bewertungen
- Radiation Hazards and Its Protection: DR - Rabia ShahDokument43 SeitenRadiation Hazards and Its Protection: DR - Rabia Shahg13818210% (1)
- AppendixDokument5 SeitenAppendixg1381821Noch keine Bewertungen
- Diagnostic Ultrasound For Postgraduates in ObstetricsDokument33 SeitenDiagnostic Ultrasound For Postgraduates in Obstetricsg1381821Noch keine Bewertungen
- The Role of Ultrasound in Obstetric and GynaecologyDokument9 SeitenThe Role of Ultrasound in Obstetric and Gynaecologyg1381821Noch keine Bewertungen
- Sonographic Mimics of Renal CalculiDokument7 SeitenSonographic Mimics of Renal Calculig1381821Noch keine Bewertungen
- Ajr 11 6559Dokument4 SeitenAjr 11 6559g1381821Noch keine Bewertungen
- Hypertrophic Pyloric Stenosis Tips and Tricks For Ultrasound DiagnosisDokument4 SeitenHypertrophic Pyloric Stenosis Tips and Tricks For Ultrasound Diagnosisg1381821Noch keine Bewertungen
- AIUM Practice GuidelineDokument12 SeitenAIUM Practice Guidelineg1381821Noch keine Bewertungen
- Ultrasound Imaging of Bowel PathologyDokument9 SeitenUltrasound Imaging of Bowel Pathologyg1381821Noch keine Bewertungen
- Introduction To CT TheoryDokument14 SeitenIntroduction To CT TheoryManoj100% (2)
- Risk Factors Pathophysiology and Management of HypertensionDokument13 SeitenRisk Factors Pathophysiology and Management of HypertensionDominggas RusunwullyNoch keine Bewertungen
- Post-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesDokument10 SeitenPost-Operative Abdominal Infections: Epidemiology, Operational Definitions, and OutcomesJared CossioNoch keine Bewertungen
- MemantineDokument7 SeitenMemantineroboNoch keine Bewertungen
- What Is Intestinal ObstructionDokument7 SeitenWhat Is Intestinal ObstructionsagerNoch keine Bewertungen
- Management of Hyperosmolar Hyperglycaemic StateDokument11 SeitenManagement of Hyperosmolar Hyperglycaemic StateTowhidulIslamNoch keine Bewertungen
- MEDDRA, PVPI, PVMF, PsMF-1Dokument28 SeitenMEDDRA, PVPI, PVMF, PsMF-1Nitin Shah100% (1)
- 17q21.31 Microdeletions FTNWDokument8 Seiten17q21.31 Microdeletions FTNWjohavenbNoch keine Bewertungen
- Blood TransfusionDokument5 SeitenBlood TransfusionMoustafa Hazzaa100% (1)
- +bashkir State Medical UniversityDokument2 Seiten+bashkir State Medical UniversityCB SharmaNoch keine Bewertungen
- The Letter of Intent To Enter PracticeDokument4 SeitenThe Letter of Intent To Enter Practicekazniels100% (1)
- Turkey Tail MushroomDokument10 SeitenTurkey Tail Mushroomjuanitos111100% (2)
- DentistDokument3 SeitenDentistuhurtuyNoch keine Bewertungen
- Cures For TinnitusDokument9 SeitenCures For TinnitusBob Skins100% (2)
- Ebook - Yoga - The Science of BreathDokument2 SeitenEbook - Yoga - The Science of BreathGabriel CiocanNoch keine Bewertungen
- Aseptic MeningitisDokument24 SeitenAseptic Meningitisidno1008100% (1)
- Drug StudyDokument4 SeitenDrug StudyYasminGianneDeOcampoBarizoNoch keine Bewertungen
- Pain ADokument19 SeitenPain Akcc2012Noch keine Bewertungen
- Msds Aplus 110 Semen AcianDokument5 SeitenMsds Aplus 110 Semen AcianWidia YpnNoch keine Bewertungen
- Raku Fire Dragon Way PDFDokument17 SeitenRaku Fire Dragon Way PDFmonipiron100% (4)
- Effectiveness of A Comprehensive Hand Hygiene Program ForDokument11 SeitenEffectiveness of A Comprehensive Hand Hygiene Program Form1k0eNoch keine Bewertungen
- NIPPVDokument35 SeitenNIPPVAnusha VergheseNoch keine Bewertungen
- Maquet Meera BrochureDokument16 SeitenMaquet Meera BrochureFeridun MADRANNoch keine Bewertungen
- A Paediatric X-Ray Exposure ChartDokument11 SeitenA Paediatric X-Ray Exposure Chartdddemourita9249Noch keine Bewertungen
- Biopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Dokument22 SeitenBiopharmaceutics and Clinical Pharmacokinetics - 20210831 - 212949Md. Abu Bakar Siddique TayefNoch keine Bewertungen
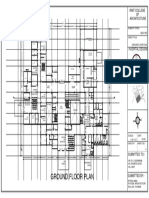
- Ground Floor Plan Sheet 2Dokument1 SeiteGround Floor Plan Sheet 2riteshNoch keine Bewertungen
- Bishinik2002 10 OriginalDokument12 SeitenBishinik2002 10 Originalalan woolardNoch keine Bewertungen
- Can Oral Sex Cause Throat CancerDokument4 SeitenCan Oral Sex Cause Throat CancerjyuldipNoch keine Bewertungen
- DolcetDokument3 SeitenDolcetConn_Casipe_8158100% (4)
- Moraxella SPP, Sphingomonas SPPDokument31 SeitenMoraxella SPP, Sphingomonas SPPDayledaniel SorvetoNoch keine Bewertungen
- Lactose Intolerance in InfantsDokument10 SeitenLactose Intolerance in InfantsflorenceNoch keine Bewertungen