Das könnte Ihnen auch gefallen
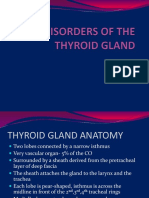
- Powerpoint: Disorders of The Thyroid GlandDokument67 SeitenPowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- Lecture Thyroid GlandDokument54 SeitenLecture Thyroid GlandMarinaNoch keine Bewertungen
- Thyroid Lumps11Dokument15 SeitenThyroid Lumps11Tareq SawanNoch keine Bewertungen
- Carcinoma of The Thyroid Gland: Regional Nodes)Dokument9 SeitenCarcinoma of The Thyroid Gland: Regional Nodes)passer byNoch keine Bewertungen
- Askep CA Paru OkDokument70 SeitenAskep CA Paru OkLisa KurniaNoch keine Bewertungen
- Thyroid Cancer Pathophysio WinjDokument4 SeitenThyroid Cancer Pathophysio WinjgeejeiNoch keine Bewertungen
- CBL Thyroid FinalDokument48 SeitenCBL Thyroid Finalimad mokalledNoch keine Bewertungen
- Thyroid Purnima 2Dokument48 SeitenThyroid Purnima 2Gaurav pareekNoch keine Bewertungen
- Thyroid Cancer: ANATOMY AND PHYSIOLOGY: The Thyroid Is A Butterfly-Shaped Gland That Sits Low OnDokument9 SeitenThyroid Cancer: ANATOMY AND PHYSIOLOGY: The Thyroid Is A Butterfly-Shaped Gland That Sits Low OnRitika RanaNoch keine Bewertungen
- Thyroid Cancer: TNM ClassificationDokument2 SeitenThyroid Cancer: TNM ClassificationEl FaroukNoch keine Bewertungen
- Solitary Thyroid NoduleDokument12 SeitenSolitary Thyroid Noduleaminappucr7Noch keine Bewertungen
- Ca ThyroidDokument36 SeitenCa ThyroidAnaswaraNoch keine Bewertungen
- Thyroid Carcinoma - DR - NishanthDokument88 SeitenThyroid Carcinoma - DR - Nishanth57- Kalanidhi mNoch keine Bewertungen
- Lung Cancer: Dr. Bhupendra Kaushik Dr. Deepti Sharma MU-2Dokument49 SeitenLung Cancer: Dr. Bhupendra Kaushik Dr. Deepti Sharma MU-2sharmadeepti1992Noch keine Bewertungen
- Testicular Tumours - Mashaal SaadDokument26 SeitenTesticular Tumours - Mashaal Saadshahryar shaukatNoch keine Bewertungen
- Tumor of Endocrine Organ: Dr. Muhartono, M.Kes, SP - PADokument80 SeitenTumor of Endocrine Organ: Dr. Muhartono, M.Kes, SP - PAreavondNoch keine Bewertungen
- Thyroid DiseasesDokument52 SeitenThyroid DiseasesNurul Sakinah Rosli100% (3)
- ThyroidectomyDokument52 SeitenThyroidectomyWindelyn Gamaro100% (4)
- ThyroidcancerDokument20 SeitenThyroidcancerReshma rsrNoch keine Bewertungen
- DR 180114164748Dokument43 SeitenDR 180114164748Hasnain ToheedNoch keine Bewertungen
- Solitary Nodule of Thyroid DR.B.VDokument18 SeitenSolitary Nodule of Thyroid DR.B.VpranapushpaNoch keine Bewertungen
- Disease of ThyroidDokument60 SeitenDisease of ThyroidMimmey YeniwNoch keine Bewertungen
- Thyroid NoduleDokument29 SeitenThyroid NoduleLavina JainNoch keine Bewertungen
- Endocrine PathologyDokument60 SeitenEndocrine PathologySingitan SiyoumNoch keine Bewertungen
- Management of Throid CancerDokument65 SeitenManagement of Throid Cancerد.صلاح مبروك خلافNoch keine Bewertungen
- Thyroid CancerDokument22 SeitenThyroid CancerHidayah JaiNoch keine Bewertungen
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDokument38 SeitenSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Report Thyroid Doc Chan SurgDokument70 SeitenReport Thyroid Doc Chan SurgShari TernolaNoch keine Bewertungen
- CBL Thyroid Pgy3Dokument48 SeitenCBL Thyroid Pgy3imad mokalledNoch keine Bewertungen
- Lec40 - Bronchogenic Carcinoma - 231205 - 120925 - 231205 - 141812Dokument37 SeitenLec40 - Bronchogenic Carcinoma - 231205 - 120925 - 231205 - 141812mahmoudsalameh192000Noch keine Bewertungen
- G4 Lung CarcinomaDokument91 SeitenG4 Lung CarcinomaYusri HarisNoch keine Bewertungen
- Thyroid Tumours: DR Khalid Azim Dept. of Surgery Islam Medical CollegeDokument37 SeitenThyroid Tumours: DR Khalid Azim Dept. of Surgery Islam Medical CollegearshmeentariqNoch keine Bewertungen
- Approach To STNDokument56 SeitenApproach To STNAbhishek VaidyaNoch keine Bewertungen
- Mohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT JuhariDokument24 SeitenMohd Helmy B Abu Bakar Farrah Hanna BT Mohd Nasir Khairunisa BT Juharimie_anumNoch keine Bewertungen
- #MediastinumDokument4 Seiten#Mediastinumameerabest100% (1)
- Lung Tumours: Bronchogenic Carcinoma Bronchial Carcinoid and Other Tumours Metastatic TumoursDokument41 SeitenLung Tumours: Bronchogenic Carcinoma Bronchial Carcinoid and Other Tumours Metastatic Tumoursvintock1979Noch keine Bewertungen
- PSGS Review 2015Dokument230 SeitenPSGS Review 2015yassercarlomanNoch keine Bewertungen
- Tumours of Thyroid GlandDokument28 SeitenTumours of Thyroid Glandjenny girlNoch keine Bewertungen
- Thyroid Carcinoma: DR Suleman Mumtaz PG 2 Ward 2Dokument81 SeitenThyroid Carcinoma: DR Suleman Mumtaz PG 2 Ward 2suleman2009Noch keine Bewertungen
- Endocrinology Revision - The Essential Hormones: Prof Julian Davis Dept of Endocrinology Manchester Royal InfirmaryDokument71 SeitenEndocrinology Revision - The Essential Hormones: Prof Julian Davis Dept of Endocrinology Manchester Royal InfirmaryAngelFire007Noch keine Bewertungen
- Hyperthyroidism 1Dokument88 SeitenHyperthyroidism 1Mamikie Vukeya100% (1)
- 11 - Part1.Neck MassesDokument51 Seiten11 - Part1.Neck MassesRashed ShatnawiNoch keine Bewertungen
- Kelainan KongenitalDokument20 SeitenKelainan KongenitalMelita GanNoch keine Bewertungen
- Surgery 1.04 Surgical Diseases of The Thyroid GlandDokument15 SeitenSurgery 1.04 Surgical Diseases of The Thyroid GlandjayaeroneNoch keine Bewertungen
- Update On Thyroid NodulesDokument57 SeitenUpdate On Thyroid NodulesHarshit SrivastavaNoch keine Bewertungen
- Radiology L2. Tuganbayeva YenglikDokument4 SeitenRadiology L2. Tuganbayeva YenglikkangliannNoch keine Bewertungen
- Parathyroid Glands: DR Priyanka ShastriDokument70 SeitenParathyroid Glands: DR Priyanka ShastriNo StradamusNoch keine Bewertungen
- Thyroid CancerDokument5 SeitenThyroid CancerJulia Rae Delos SantosNoch keine Bewertungen
- Thyroid Diseases 3 NeoplasmDokument30 SeitenThyroid Diseases 3 NeoplasmSolomon Fallah Foa SandyNoch keine Bewertungen
- Pediatric Abdominal TumorsDokument27 SeitenPediatric Abdominal TumorsDlman JamalNoch keine Bewertungen
- Presentation Small Cell Lung CancerDokument59 SeitenPresentation Small Cell Lung Cancerprudhviraj mNoch keine Bewertungen
- Management of Thyroid Nodule Setela DirubaDokument38 SeitenManagement of Thyroid Nodule Setela DirubaahmadfauzanarifaniNoch keine Bewertungen
- Benign Malignant LarynxDokument28 SeitenBenign Malignant LarynxfaizNoch keine Bewertungen
- Messages in Surgical Approach To Endocrine Glands: Prof. Ayman Mismar 17/ 8/ 2019Dokument46 SeitenMessages in Surgical Approach To Endocrine Glands: Prof. Ayman Mismar 17/ 8/ 2019AmyandNoch keine Bewertungen
- Endocrine System:SurgeriesDokument8 SeitenEndocrine System:Surgeriesasheehan17Noch keine Bewertungen
- Thyroid MalignancyDokument18 SeitenThyroid MalignancyAmr AbualrubNoch keine Bewertungen
- Benign Thyroid DiseasesDokument11 SeitenBenign Thyroid Diseasesj6r4qvkrkzNoch keine Bewertungen
- Thyroid CancerDokument28 SeitenThyroid CancerIoana CozmaNoch keine Bewertungen
- Alert Medical Series: Internal Medicine Alert I, II, IIIVon EverandAlert Medical Series: Internal Medicine Alert I, II, IIINoch keine Bewertungen
- Atherosclerosis. Biochemical Modifications in Acute Coronary SyndromeDokument12 SeitenAtherosclerosis. Biochemical Modifications in Acute Coronary Syndromej.doe.hex_87Noch keine Bewertungen
- Aplast AnDokument9 SeitenAplast Anj.doe.hex_87Noch keine Bewertungen
- Nutrition in InfantDokument7 SeitenNutrition in Infantj.doe.hex_87Noch keine Bewertungen
- Namaz - The Health BenefitsDokument130 SeitenNamaz - The Health Benefitsj.doe.hex_87100% (1)
- Lecture2c MdsyndromesDokument2 SeitenLecture2c Mdsyndromesj.doe.hex_87Noch keine Bewertungen
- Svaritm 2010Dokument26 SeitenSvaritm 2010j.doe.hex_87Noch keine Bewertungen
- Understanding The 12 - Lead ECG, Part IIDokument11 SeitenUnderstanding The 12 - Lead ECG, Part IIj.doe.hex_87Noch keine Bewertungen
- Understanding The 12 - Lead ECG, Part 1Dokument9 SeitenUnderstanding The 12 - Lead ECG, Part 1j.doe.hex_87Noch keine Bewertungen
- Aplastic Anemia, 2008Dokument10 SeitenAplastic Anemia, 2008j.doe.hex_87Noch keine Bewertungen
- Studies Suggest That Myocarditis Is A: Important Causes of MyocarditisDokument11 SeitenStudies Suggest That Myocarditis Is A: Important Causes of MyocarditisCristina Georgiana CoticăNoch keine Bewertungen
- Cardiac Imaging TechniquesDokument86 SeitenCardiac Imaging Techniquesj.doe.hex_87Noch keine Bewertungen
- Water and Electrolytes DisturbancesDokument63 SeitenWater and Electrolytes Disturbancesj.doe.hex_87Noch keine Bewertungen
- The Liver: Methods of ExaminationDokument49 SeitenThe Liver: Methods of Examinationj.doe.hex_87Noch keine Bewertungen
- Radiology - Imaging of The ThoraxDokument49 SeitenRadiology - Imaging of The Thoraxj.doe.hex_87Noch keine Bewertungen
- Radiology - Imaging of The ThoraxDokument49 SeitenRadiology - Imaging of The Thoraxj.doe.hex_87Noch keine Bewertungen
- Methods of ExaminationDokument56 SeitenMethods of Examinationj.doe.hex_87Noch keine Bewertungen
- Hydatid Disease: or Iceberg SignDokument53 SeitenHydatid Disease: or Iceberg Signj.doe.hex_87Noch keine Bewertungen
- Lung CancerDokument19 SeitenLung Cancerj.doe.hex_87Noch keine Bewertungen
- Lionte Cor Pulmonale2010Dokument11 SeitenLionte Cor Pulmonale2010j.doe.hex_87Noch keine Bewertungen
- Powerpoint: Chronic Inflammatory DisordesDokument55 SeitenPowerpoint: Chronic Inflammatory Disordesj.doe.hex_87Noch keine Bewertungen
- Powerpoint: Gall Stone Disease and Related DisordersDokument70 SeitenPowerpoint: Gall Stone Disease and Related Disordersj.doe.hex_8767% (3)
- Lecture 1 Chest TraumaDokument19 SeitenLecture 1 Chest Traumaj.doe.hex_870% (1)
- Powerpoint: Liver Surgical DiseasesDokument95 SeitenPowerpoint: Liver Surgical Diseasesj.doe.hex_8792% (12)
- Endocrinology Pharmacology: Hormone Agonists, Antagonists & ModulatorsDokument151 SeitenEndocrinology Pharmacology: Hormone Agonists, Antagonists & Modulatorsj.doe.hex_87100% (1)
- Machine Learning and Supply Chain Management - ADokument5 SeitenMachine Learning and Supply Chain Management - AAhmed AbassNoch keine Bewertungen
- 9709 w05 Ms 2Dokument5 Seiten9709 w05 Ms 2michael hengNoch keine Bewertungen
- Listening 3b Skills Test 1aDokument3 SeitenListening 3b Skills Test 1aPticaSelicaNoch keine Bewertungen
- List of ErpDokument2 SeitenList of Erpnavyug vidyapeeth trust mahadNoch keine Bewertungen
- Mind'S Nest Review Center Inc.,: Criteria of A Good Research Problem: Easibility Nterest EsearchabilityDokument21 SeitenMind'S Nest Review Center Inc.,: Criteria of A Good Research Problem: Easibility Nterest EsearchabilitySherlyn Pedida100% (1)
- 1609 Um009 - en PDokument34 Seiten1609 Um009 - en PAnonymous VKBlWeyNoch keine Bewertungen
- Pengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahDokument13 SeitenPengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahAhmad HerdandiNoch keine Bewertungen
- Clay and Shale, Robert L VirtaDokument24 SeitenClay and Shale, Robert L VirtaRifqi Brilyant AriefNoch keine Bewertungen
- Breaking News EnglishDokument13 SeitenBreaking News English32. Nguyễn OanhNoch keine Bewertungen
- Future Scope and ConclusionDokument13 SeitenFuture Scope and ConclusionGourab PalNoch keine Bewertungen
- IGCSE Religious Studies (Edexcel - 2009 - Be Careful Not To Choose The New' IGCSE)Dokument8 SeitenIGCSE Religious Studies (Edexcel - 2009 - Be Careful Not To Choose The New' IGCSE)Robbie TurnerNoch keine Bewertungen
- Wayne A. Thorp - Analyzing Supply & Demand Using Point & Figure Charts PDFDokument5 SeitenWayne A. Thorp - Analyzing Supply & Demand Using Point & Figure Charts PDFSrinivasNoch keine Bewertungen
- Q4L6 Properties of KiteDokument8 SeitenQ4L6 Properties of KiteAltheus Miguel Dela CruzNoch keine Bewertungen
- Upsa Y5 2023Dokument8 SeitenUpsa Y5 2023Faizal AzrinNoch keine Bewertungen
- Course: Consumer Behaviour: Relaunching of Mecca Cola in PakistanDokument10 SeitenCourse: Consumer Behaviour: Relaunching of Mecca Cola in PakistanAnasAhmedNoch keine Bewertungen
- Al-Ahbash Evolution and BeliefsDokument4 SeitenAl-Ahbash Evolution and BeliefskaptenzainalNoch keine Bewertungen
- Arithmetic Mean PDFDokument29 SeitenArithmetic Mean PDFDivya Gothi100% (1)
- A Seventh-Day Adventist Philosophy of MusicDokument5 SeitenA Seventh-Day Adventist Philosophy of MusicEddy IsworoNoch keine Bewertungen
- Negotiation SimulationDokument11 SeitenNegotiation SimulationJade Arbee BarbosaNoch keine Bewertungen
- Cottrell Park Golf Club 710Dokument11 SeitenCottrell Park Golf Club 710Mulligan PlusNoch keine Bewertungen
- Sa Inc HCP English d10840Dokument64 SeitenSa Inc HCP English d10840Ayu AfiantyNoch keine Bewertungen
- 1.4 BG00381946 - ADokument1 Seite1.4 BG00381946 - AAnand KesarkarNoch keine Bewertungen
- IELTS Materials ReadingDokument9 SeitenIELTS Materials ReadingßläcklìsètèdTȜè0% (1)
- B - ELSB - Cat - 2020 PDFDokument850 SeitenB - ELSB - Cat - 2020 PDFanupamNoch keine Bewertungen
- AH Business-Management All 2011Dokument11 SeitenAH Business-Management All 2011Sanam PuriNoch keine Bewertungen
- Structure of An Atom Revision PaperDokument5 SeitenStructure of An Atom Revision PaperZoe Kim ChinguwaNoch keine Bewertungen
- Unit 8 Atomic Fluorescence Spectrometry PDFDokument23 SeitenUnit 8 Atomic Fluorescence Spectrometry PDFCh AswadNoch keine Bewertungen
- Model Questions and Answers Macro EconomicsDokument14 SeitenModel Questions and Answers Macro EconomicsVrkNoch keine Bewertungen
- ErtlDokument64 SeitenErtlManpreet SinghNoch keine Bewertungen
- Jahnteller Effect Unit 3 2017Dokument15 SeitenJahnteller Effect Unit 3 2017Jaleel BrownNoch keine Bewertungen