Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Cryptogenic StrokeDokument52 SeitenCryptogenic Strokemrabhilekh100% (1)
- Dental Management Medically Compromised Patient 9th Little Test BankDokument5 SeitenDental Management Medically Compromised Patient 9th Little Test BankSaifoqq100% (1)
- 25) Aetiology and Pathogenesis of Valvular Heart DiseaseDokument34 Seiten25) Aetiology and Pathogenesis of Valvular Heart DiseaseGurrajvin Singh0% (1)
- #9 Ie 8 PDFDokument8 Seiten#9 Ie 8 PDFOmar BasimNoch keine Bewertungen
- Underground Clinical Vignettes Microbiology IDokument120 SeitenUnderground Clinical Vignettes Microbiology IGeorge HananiaNoch keine Bewertungen
- Larynx (Voice Box)Dokument59 SeitenLarynx (Voice Box)alfaz lakhaniNoch keine Bewertungen
- 2016 UPH Pathology Review TemploDokument203 Seiten2016 UPH Pathology Review TemploSherlock Holmes33% (3)
- Soal 5Dokument31 SeitenSoal 5Agustinus FatollaNoch keine Bewertungen
- Management of Patients With Special Health Care NeedsDokument30 SeitenManagement of Patients With Special Health Care NeedsEslam HafezNoch keine Bewertungen
- William Osler El Hombre y Sus Descripciones PDFDokument10 SeitenWilliam Osler El Hombre y Sus Descripciones PDFDaniel JimenezNoch keine Bewertungen
- Chapter 36: Inflammatory and Structural Heart Disorders Harding: Lewis's Medical-Surgical Nursing, 11th EditionDokument12 SeitenChapter 36: Inflammatory and Structural Heart Disorders Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaNoch keine Bewertungen
- Meningitis and Acute MeningococcemiaDokument16 SeitenMeningitis and Acute Meningococcemiaalfaz lakhaniNoch keine Bewertungen
- ROLL No.43Dokument18 SeitenROLL No.43alfaz lakhaniNoch keine Bewertungen
- InfluenzaDokument22 SeitenInfluenzaalfaz lakhaniNoch keine Bewertungen
- Hippocrates Was Probably The First Malariologist. by 400BC, He Described The Various Malaria Fevers ofDokument3 SeitenHippocrates Was Probably The First Malariologist. by 400BC, He Described The Various Malaria Fevers ofalfaz lakhaniNoch keine Bewertungen
- The Concept of Epidemic ProcessDokument8 SeitenThe Concept of Epidemic Processalfaz lakhaniNoch keine Bewertungen
- DysenteryDokument2 SeitenDysenteryalfaz lakhaniNoch keine Bewertungen
- Foreign Bodies in Otorhinology: DR Yojana Sharma Assosiate Professor Dept of ENT PSMC, KaramsadDokument32 SeitenForeign Bodies in Otorhinology: DR Yojana Sharma Assosiate Professor Dept of ENT PSMC, Karamsadalfaz lakhaniNoch keine Bewertungen
- General EpidermiologyDokument4 SeitenGeneral Epidermiologyalfaz lakhaniNoch keine Bewertungen
- Intestinal InfectionDokument1 SeiteIntestinal Infectionalfaz lakhaniNoch keine Bewertungen
- Headache & Facial Pain: An ENT AspectDokument11 SeitenHeadache & Facial Pain: An ENT Aspectalfaz lakhaniNoch keine Bewertungen
- Diseases of Oral CavityDokument3 SeitenDiseases of Oral Cavityalfaz lakhaniNoch keine Bewertungen
- Lower Motor Neuron (LMN) Facial Palsy: Department of ENTDokument32 SeitenLower Motor Neuron (LMN) Facial Palsy: Department of ENTalfaz lakhani100% (1)
- Presentation By: DR Yojana SharmaDokument15 SeitenPresentation By: DR Yojana Sharmaalfaz lakhaniNoch keine Bewertungen
- CsomDokument22 SeitenCsomalfaz lakhaniNoch keine Bewertungen
- Diseases of Oral CavityDokument3 SeitenDiseases of Oral Cavityalfaz lakhaniNoch keine Bewertungen
- Diseases of Oral CavityDokument3 SeitenDiseases of Oral Cavityalfaz lakhaniNoch keine Bewertungen
- Anatomy of Oral CavityDokument8 SeitenAnatomy of Oral Cavityalfaz lakhaniNoch keine Bewertungen
- 30 - Funct - Dis of Dig - Syst.Dokument52 Seiten30 - Funct - Dis of Dig - Syst.alfaz lakhaniNoch keine Bewertungen
- Clinical Management Protocol and Infection Control GuidelinesDokument16 SeitenClinical Management Protocol and Infection Control Guidelinesalfaz lakhaniNoch keine Bewertungen
- Chronic Gastritis. Ulcer of Stomach and DuodenumDokument39 SeitenChronic Gastritis. Ulcer of Stomach and Duodenumalfaz lakhaniNoch keine Bewertungen
- Tasbih Benefits Compiled by KabirDokument9 SeitenTasbih Benefits Compiled by Kabiralfaz lakhaniNoch keine Bewertungen
- Forensic Medicine Toxicology Last Minute ReviewDokument102 SeitenForensic Medicine Toxicology Last Minute Reviewsruthimeena6891Noch keine Bewertungen
- Microbiology of CVSDokument44 SeitenMicrobiology of CVSsultan khabeebNoch keine Bewertungen
- Sas 13Dokument5 SeitenSas 13Sistine Rose LabajoNoch keine Bewertungen
- Mitral Valve ReplacementDokument44 SeitenMitral Valve ReplacementYusardi R Pradana100% (1)
- Aortic RegurgitationDokument16 SeitenAortic Regurgitationrobby zayendraNoch keine Bewertungen
- Professor Graham R V Hughes MD FRCPDokument99 SeitenProfessor Graham R V Hughes MD FRCPhastuti tajuddinNoch keine Bewertungen
- Fishbein 2019Dokument8 SeitenFishbein 2019hawk.man8Noch keine Bewertungen
- 2019 Batch PapersDokument21 Seiten2019 Batch PaperssaranshjainworkNoch keine Bewertungen
- CASE STUDY - Infective EndocarditisDokument6 SeitenCASE STUDY - Infective EndocarditisDudil GoatNoch keine Bewertungen
- Pyrexia of Unknown OriginDokument81 SeitenPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- Management of Patients With Systemic Diseases in Oral SurgeryDokument42 SeitenManagement of Patients With Systemic Diseases in Oral SurgeryRichard Starr100% (2)
- Ug Infective Endocarditis SubmitDokument49 SeitenUg Infective Endocarditis SubmitAhmed FaizalNoch keine Bewertungen
- Case Study 4 Bacterial EndocarditisDokument13 SeitenCase Study 4 Bacterial Endocarditisintrovoyz041Noch keine Bewertungen
- New Patients EndocarditisDokument1 SeiteNew Patients EndocarditisnayanastarNoch keine Bewertungen
- 8.29.06 Staphlococcal BacteremiaDokument41 Seiten8.29.06 Staphlococcal BacteremiaVaibhav KaroliyaNoch keine Bewertungen
- Infective EndocarditisDokument10 SeitenInfective EndocarditisShrests SinhaNoch keine Bewertungen
- Cardio Nursing - Course Audit 2Dokument320 SeitenCardio Nursing - Course Audit 2Ciella Dela CruzNoch keine Bewertungen
- Rare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesDokument3 SeitenRare and Fatal Complication of Infective Endocarditis: Emergency Case SeriesVika DamayNoch keine Bewertungen
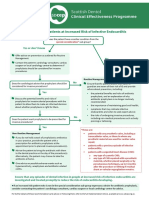
- SDCEP Antibiotic Prophylaxis Summary FlowchartDokument1 SeiteSDCEP Antibiotic Prophylaxis Summary FlowchartMahmoud EladawyNoch keine Bewertungen
- Hemant Ashraf Waseem - 1Dokument17 SeitenHemant Ashraf Waseem - 1Kunal BhamareNoch keine Bewertungen
- Case Presentation: Infective EndocarditisDokument13 SeitenCase Presentation: Infective EndocarditisHillaryNoch keine Bewertungen